The purpose of this blog is to answer 5 questions:
1. What is a disc herniation?
2. Can a disc herniation heal?
3. Do MRIs tell the whole story?
4. Do you NEED surgery?
5. What can you do for yourself?
Do you have new, lingering, or recurring low back pain that’s stopping you from doing the things you enjoy or keeping you from feeling like yourself? Check out our Low Back Resilience Program!
What is a disc herniation?
The intervertebral disc, separating one vertebral body from another, consists of the nucleus pulposus and annulus fibrosus. It also has two vertebral endplates that connect the disc to the bones above and below, making it impossible for the disc to slip. The disc promotes movement, shock absorption, and the transfer of load.

According to Fardon et al in 2014, a disc herniation is defined as the “localized or focal displacement of disc material beyond the normal margin of the intervertebral disc space,” which may be further classified as a protrusion, extrusion, or sequestration. A bulging disc may also be seen on imaging, but is not considered a form of herniation.

It is possible for a disc herniation to contribute to the irritation of a nerve in your low back, which is why you’re likely reading this blog.
Can a disc herniation heal?
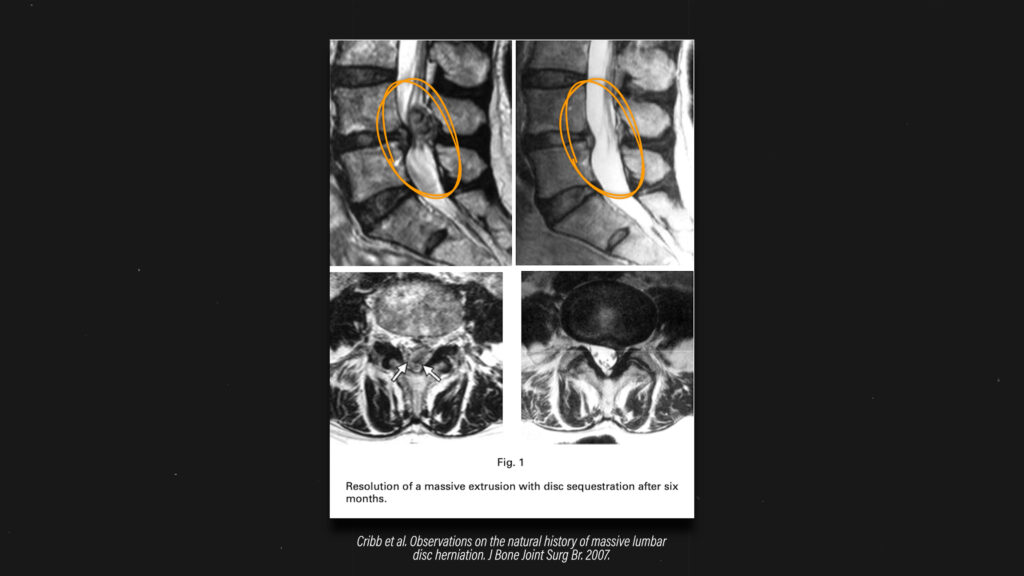
Fortunately, a disc herniation can heal on its own. This has been supported by systematic reviews by Chiu et al in 2015, Zhong et al in 2017, and Wang et al in 2020. Here’s an image from a case example in which the disc herniation significantly regressed/resorbed over time.
Do MRIs tell the whole story?
Despite disc herniations being able to completely heal on their own, MRIs don’t always tell the whole story. Here are 4 things you should know:
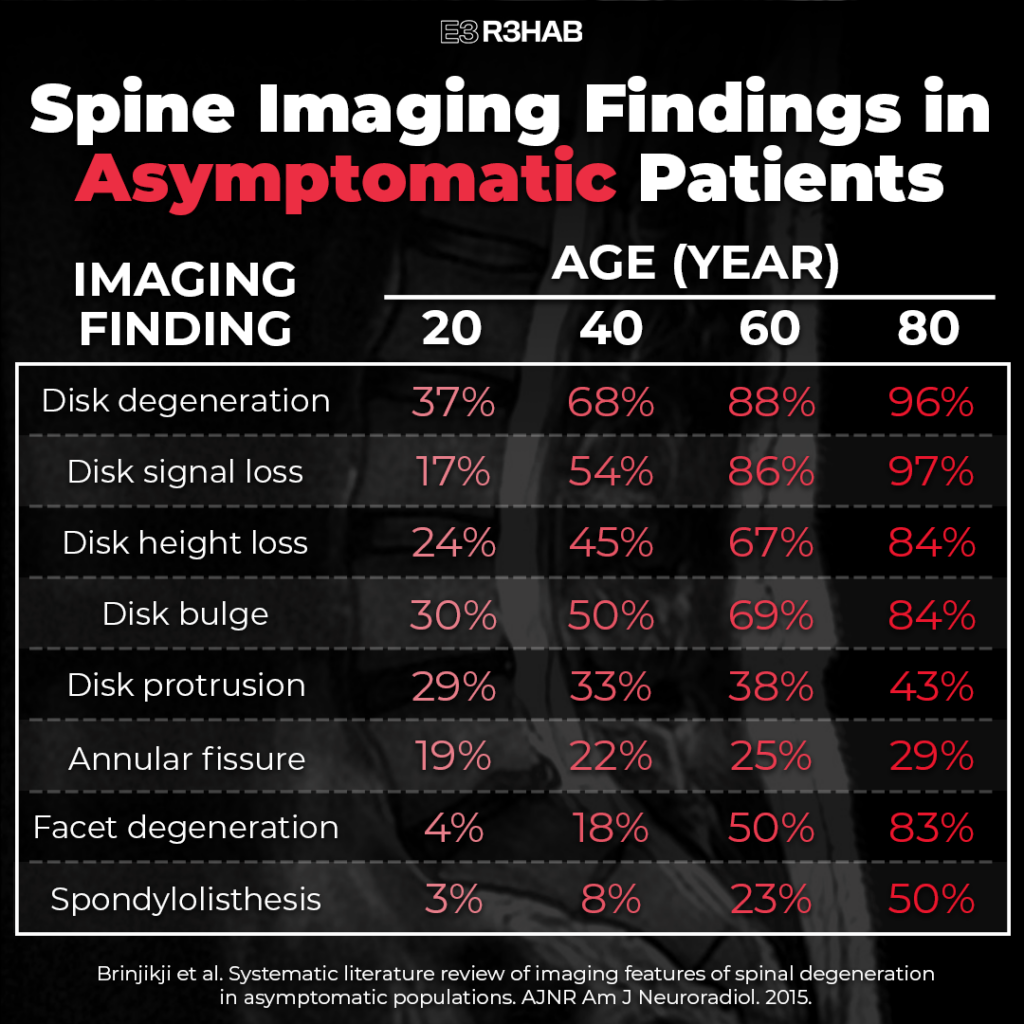
- “Abnormalities” are common in the asymptomatic population. A systematic review by Brinjikji et al in 2015 found that 29% of asymptomatic 20 year olds have a disc protrusion and this number increases as we age. The same is true for disc bulges.
- Size doesn’t always matter, at least for disc herniations. Karppinen et al in 2001, Benson et al in 2010, and Gupta et al in 2020 found that even large disc herniations can heal, and the size or degree of herniation doesn’t necessarily correlate with symptoms.
- The amount of regression or resorption of the disc herniation isn’t always associated with clinical outcomes. Fraser et al in 1995, Benson et al in 2010, and Barzouhi et al in 2013 found that you can become asymptomatic despite the disc herniation still being present on MRI.
- Symptoms are complex and multifactorial. Karppinen et al in 2001 reported that more compression of a nerve on MRI doesn’t necessarily mean worse symptoms. Rijn et al in 2006 also found that it’s possible to have compression of a nerve with no symptoms at all.
Do you NEED surgery?
The information up to this point informs us that MOST people will NOT require surgery, and this is supported by the research.
When comparing surgical to non-surgical management of sciatica-like symptoms related to disc herniations, a systematic review by Ferndandez et al in 2016 suggests that outcomes are similar between the groups in the long-term. When surgery is performed, Peul et al in 2007 and Overdevest et al in 2014 demonstrated that it may lead to a greater improvement in pain, recovery of function, and reduction in disability in the short-term. However, results are comparable to non-surgical management after 1 year.
Surgery may be indicated in some cases, such as when severe or progressive neurologic deficits are present, but non-operative management is usually the first recommendation. In fact, in line with several medical guidelines, Deyo and Mirza suggest that MRI should be discouraged unless symptoms are not improving after attempting 4-6 weeks of nonsurgical management. An early MRI can have negative consequences, such as increased costs and unnecessary treatment.
What can you do for yourself?
I’m going to break it up into 3 categories:
- Posture and Positions. Identify if certain postures, positions, or movements aggravate your symptoms. For example, some people find that sitting for prolonged periods of time is problematic. You could minimize or reduce the time spent sitting. And make sure to consider your entire day – time spent driving, working, watching Netflix, scrolling Instagram, etc. Identify those aggravating postures, positions, or movements and determine if you can minimize, reduce, or modify them.
- Exercise. Despite what you may have heard, seen, or read, there is no BEST exercise. This is actually a good thing because it means you get to choose what you like to do or what feels good for you.
- Lifestyle Modifications. Living a healthier lifestyle is always going to be better for healing – sleeping well, eating well, exercising regularly, not smoking, etc. Easy to do in theory, harder to do in practice. I recommend picking one thing to change that’s doable for you. For example, commit to performing three 10 minute walks per day. This might even be a way to break up those periods of prolonged inactivity or sitting.

I know these recommendations sound basic, but all you’re trying to do is create the optimal environment for healing while the sophisticated organism that is your human body does what it’s supposed to do.
Summary
In summary, disc herniations CAN heal, MRIs don’t always tell the full story, surgery is not required in MOST cases, and there are several strategies you can use to help manage your symptoms.