The purpose of this blog is to discuss the diagnosis and clinical course of frozen shoulder, exercise guidelines, and briefly review other management strategies for rehabilitation.
Looking for rehab or performance programs? Check out our store here!
What is Frozen Shoulder?
Frozen shoulder typically presents with shoulder pain and a progressive loss of both active and passive shoulder movement.

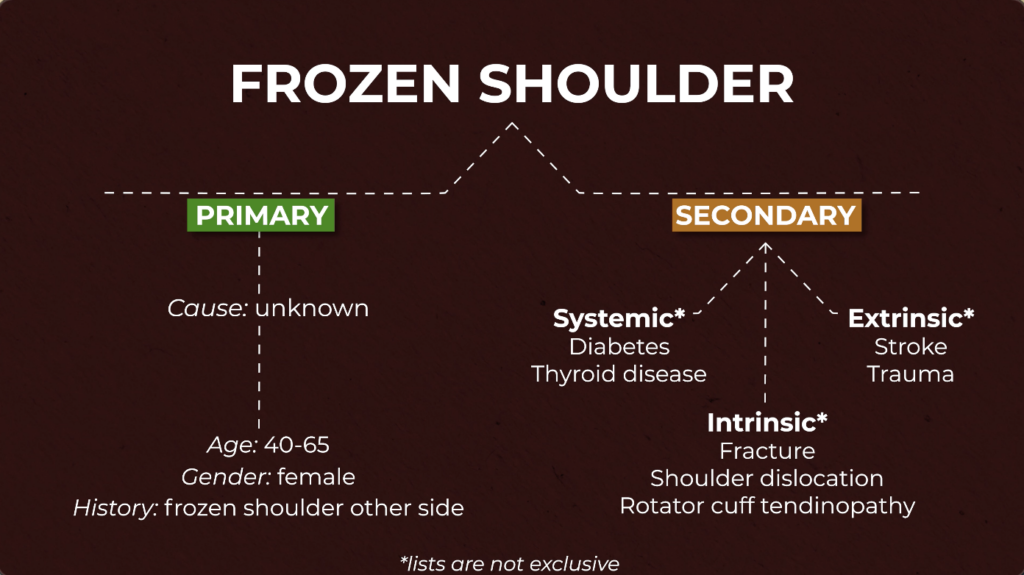
There are generally two types of frozen shoulder: primary and secondary.
With primary frozen shoulder, the exact cause is unknown, and that is why it is often described as idiopathic. However it is generally more prevalent in those who are 40-65 year olds, female, and who previously had frozen shoulder on the opposite side.
Secondary frozen shoulder can be associated with diabetes, thyroid disease, stroke, trauma, and various shoulder pathologies.
It was originally believed that adhesions, fibrosis, and inflammation of the shoulder capsule and surrounding structures were sole contributors to this pain and loss of motion. Hence its other name, adhesive capsulitis.
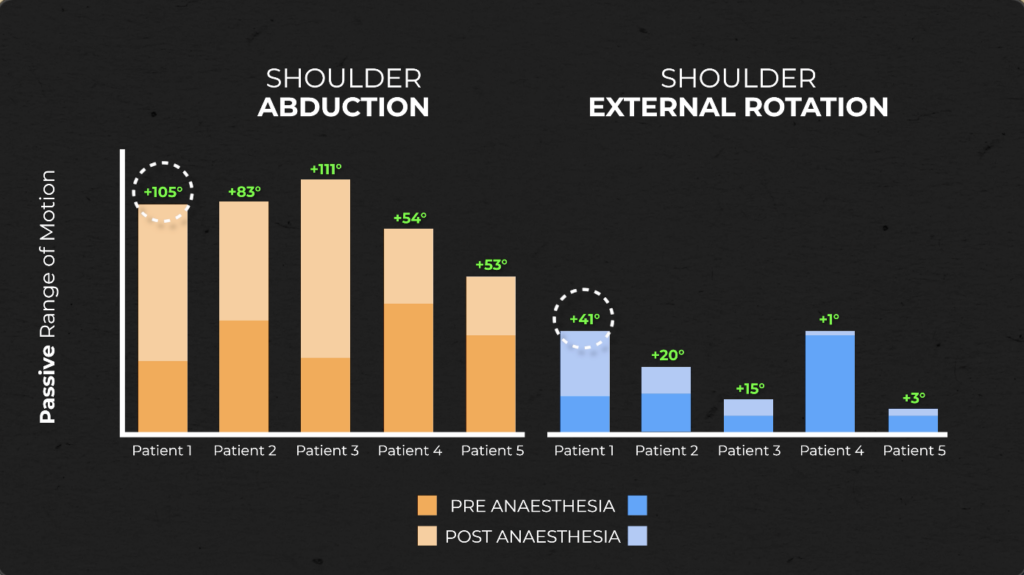
However, a popular study by Hollman et al. 2018, found that in 5 patients with frozen shoulder, passive shoulder range of motion significantly improved after the administration of general anesthesia.
All 5 patients saw a significant increase in shoulder abduction while three demonstrated an increase in external rotation. One patient even saw an increase up to 105° of shoulder abduction and 41° in shoulder external rotation!
This information tells us that frozen shoulder may not be solely as structural as once thought. While inflammation and restriction in the capsule and adjacent tissues still play a role (especially as immobilization progresses), it is important to understand that muscle guarding and pain are likely major contributors to the movement restrictions seen in some individuals with frozen shoulder.
Note: This is a key reason why aggressive, painful stretching focused on “breaking up” shoulder adhesions is not necessary in rehabilitation. Stretching can still be implemented, but follow the pain guidelines reviewed in the “Exercise Guidelines” section.
Diagnosis
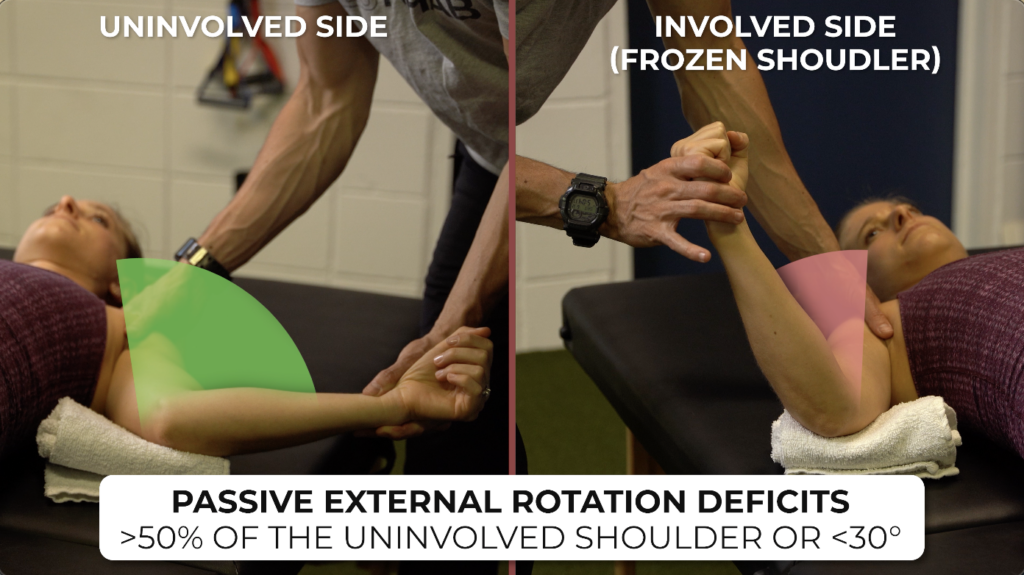
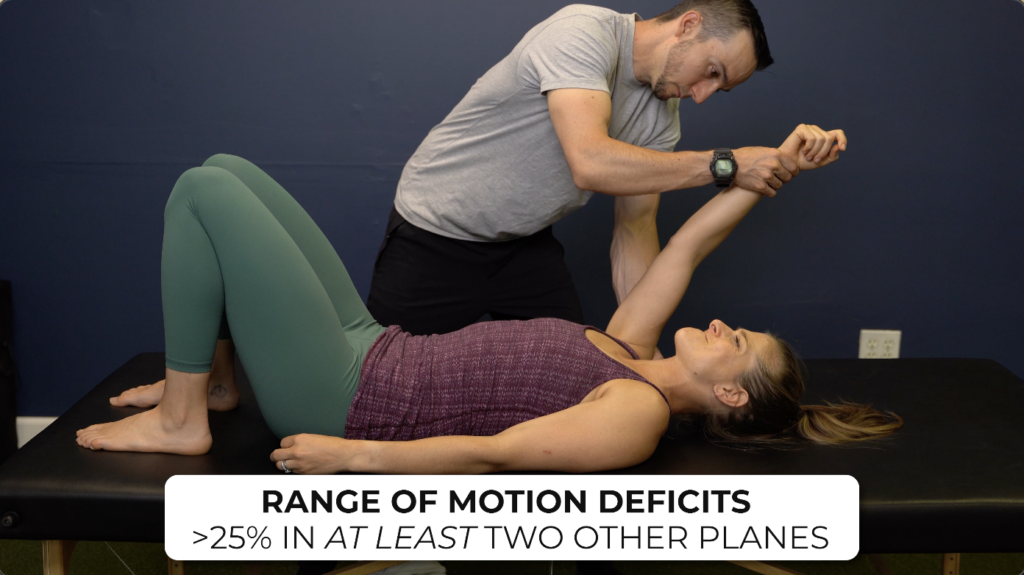
Frozen shoulder will present with passive external rotation loss that is greater than 50% of the uninvolved shoulder or less than 30°. This measurement is taken with the shoulder in neutral, or arm at the side.
Additionally, it will also have deficits in range of motion of greater than 25% in 2 other planes. For example, shoulder flexion and abduction may be limited by 25% compared to the other shoulder.
It is worth noting that other conditions can present similarly, such as severe osteoarthritis, acute bursitis, rotator cuff tendinopathy, fracture, and posterior fixed shoulder dislocation, to name a few.
X rays are not necessary, but can help rule in or out other conditions, such as severe osteoarthritis or a dislocation.
Clinical Course & Expectations
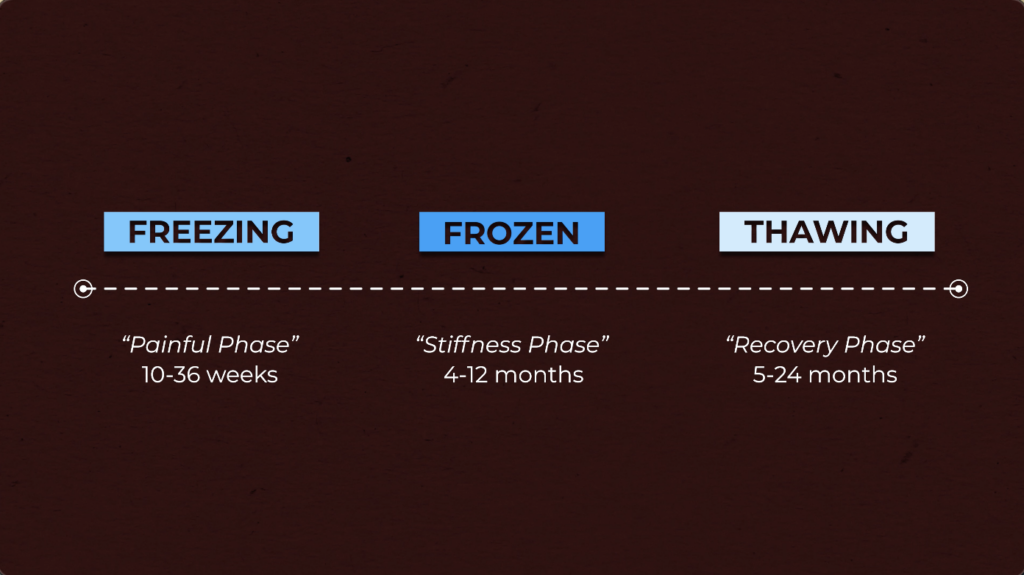
It has been proposed that frozen shoulder progresses through a self-limiting, natural history of 3 separate stages: freezing, frozen and thawing. (Grey, Reeves, Simmonds).
Each stage was named based on symptom presentation and provided a timeline.
- Freezing was termed the “painful phase” and lasted 10 to 36 weeks.
- Frozen was termed the “stiffness phase” and lasted 4 to 12 months.
- And thawing was termed the “recovery phase” and lasted anywhere from 5 to 24 months.
However, there are 2 reasons why these phases might not be the most appropriate to use.
First, they imply a natural history, meaning it progresses through different phases, ultimately leading to full recovery without treatment.
However, a 2017 systematic review by Wong et al. 2017 found that “there was in fact no evidence to support this theory.” Furthermore “expectations of eventual “thawing” leading to complete recovery without treatment may lead patients to delay or forego treatment.”
And second, these timelines may set a false expectation for the duration of symptoms. An article by Hand et al. found that some patients reported mild/moderate and severe shoulder symptoms anywhere from 2 to 7 or more years after initial onset of frozen shoulder.
The big takeaway here is that symptoms will improve and functional limitations will get better, but it will take time and effort. Frozen shoulder is a slow moving condition with extremely variable and unpredictable time frames. Rather than setting a concrete timeline for recovery, focus on making objective progress over a period of weeks to months. For example, can you reach your arm overhead further? Or are you able to increase weight or reps with different exercises?
Note: If someone tells you they received a given treatment and it immediately fixed their frozen shoulder, they likely did not have frozen shoulder. So be very cautious on any claims that provide a quick fix.
Exercise Guidelines for Frozen Shoulder
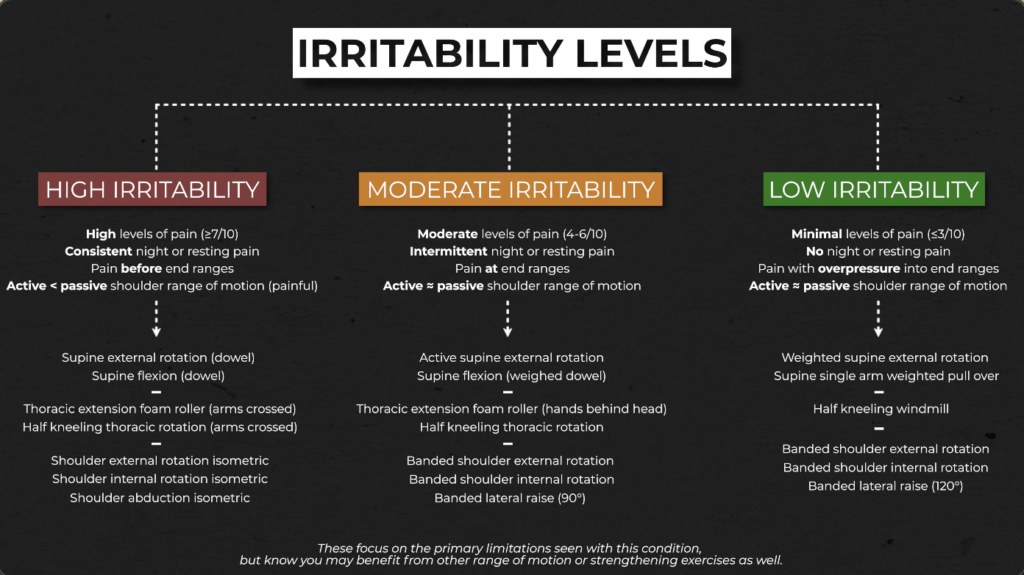
Exercises should be chosen based on your irritability levels. There are 3 levels: high, moderate, and low.
High irritability is generally characterized by:
- High levels of pain (≥7/10).
- Consistent night or resting pain.
- Pain occuring before end ranges of shoulder movements.
- Active shoulder range of motion that is significantly less than passive range of motion secondary to pain.
Moderate irritability is generally characterized by:
- Moderate levels of pain (4-6/10)
- Intermittent night or resting pain.
- Pain occuring at end ranges of shoulder movements
- Active shoulder range of motion that is similar to passive range of motion.
And low irritability is generally characterized by:
- Minimal levels of pain (≤3/10).
- No night or resting pain
- Pain occurring with overpressures into end ranges of shoulder movements.
- Active shoulder range of motion that is similar to passive range of motion.
Exercises will include options for improving shoulder flexion and external rotation range of motion; thoracic mobility since this can further help improve shoulder range of motion and function (Barrett et al., Miyashita et al., Suzuki et al., Lewis et al.); and shoulder strength to help maximize outcomes and address another deficit commonly seen in frozen shoulder.
Note: These exercise suggestions are based on the primary limitations seen with this condition, but you may benefit from other range of motion or strengthening exercises as well.
High Irritability.
Since pain is already high, focus on performing exercises relatively pain-free, or within comfort.
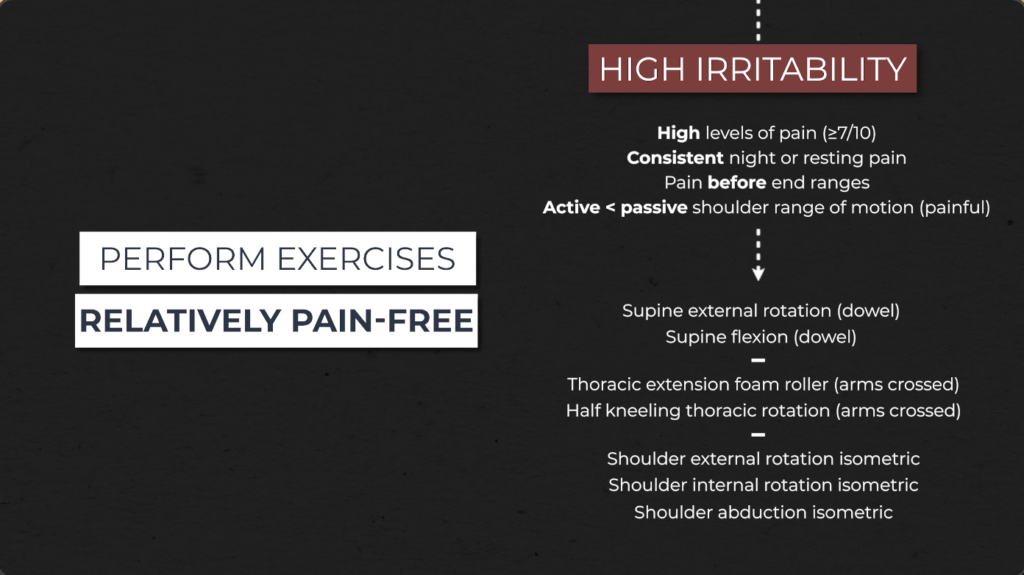
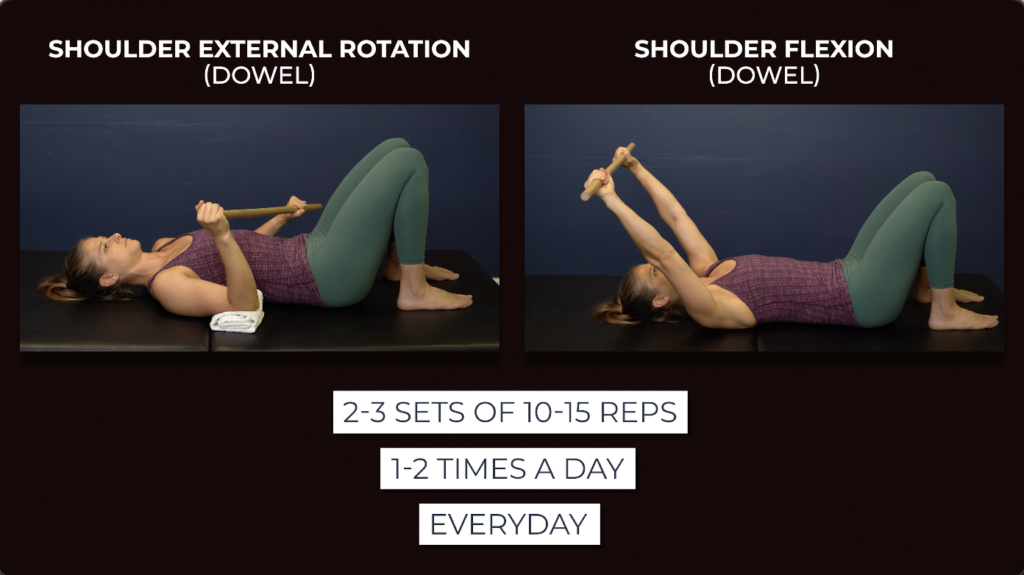
Supine external rotation using a dowel. Lie on your back and place the involved shoulder at your side, supported on a towel or object for comfort, and your elbow bent to 90°. Holding a stick or dowel, use the non involved side to move your shoulder in and out of as much external rotation as tolerable.

Supine shoulder flexion with a dowel. Lie on your back and hold a dowel or stick with both hands up toward the ceiling. Slowly move your arms overhead as far as tolerable and then return to the start and repeat.

For either of these options, use as much as assistance from the uninvolved side as needed and perform for 2-3 sets of 10-15 repetitions, 1-2x a day, everyday or within tolerance.
For thoracic mobility, here are 2 options: one for thoracic extension and one for rotation.
Thoracic extension on a foam roller. Place a foam roller across your thoracic spine, or middle back, and support your head with your uninvolved arm while crossing the involved arm over your chest. Extend your spine back as far as comfortable and then return to a flexed position. Repeat this motion of extension and flexion, along multiple points of the thoracic spine.

Half kneeling thoracic rotation with arms crossed. Rotate over the “up” knee, twisting through your middle and upper back.

For either of these thoracic mobility exercises, perform for 2-3 sets of 10-12 repetitions, 1-2x a day, every day or within tolerance.

And finally, 3 options for shoulder strength: shoulder internal rotation, external rotation and abduction isometrics.
If you have high irritability, isometrics may be a good starting point, since these will activate the muscles without moving the joint, allow you to self-select your level of intensity, and may help reduce pain.
Internal rotation isometric. Stand in front of a door frame or another immovable object with your upper arm at your side, elbow bent to 90°, and lower arm straight ahead. Press inward, without moving your arm, shoulder or body.
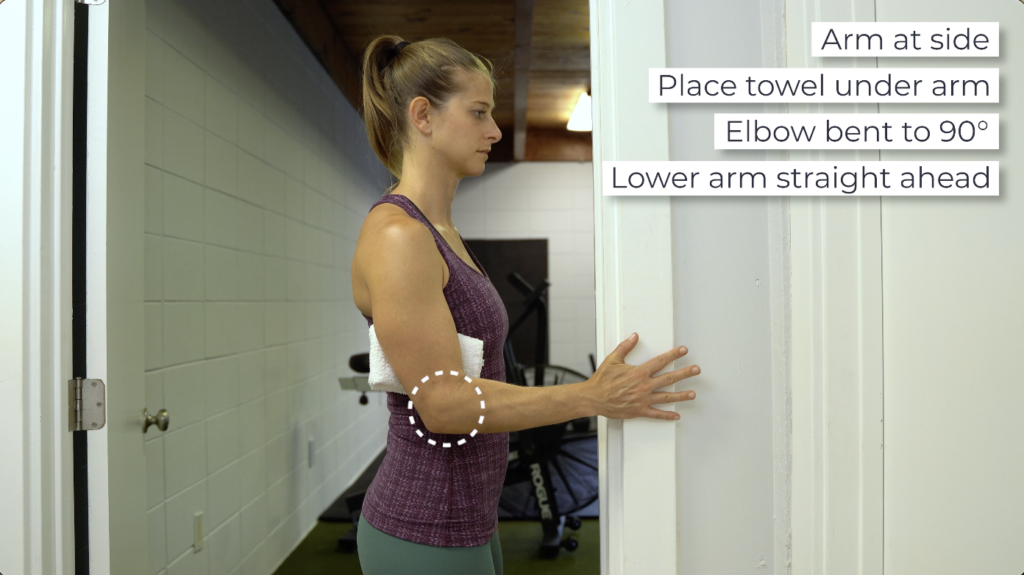
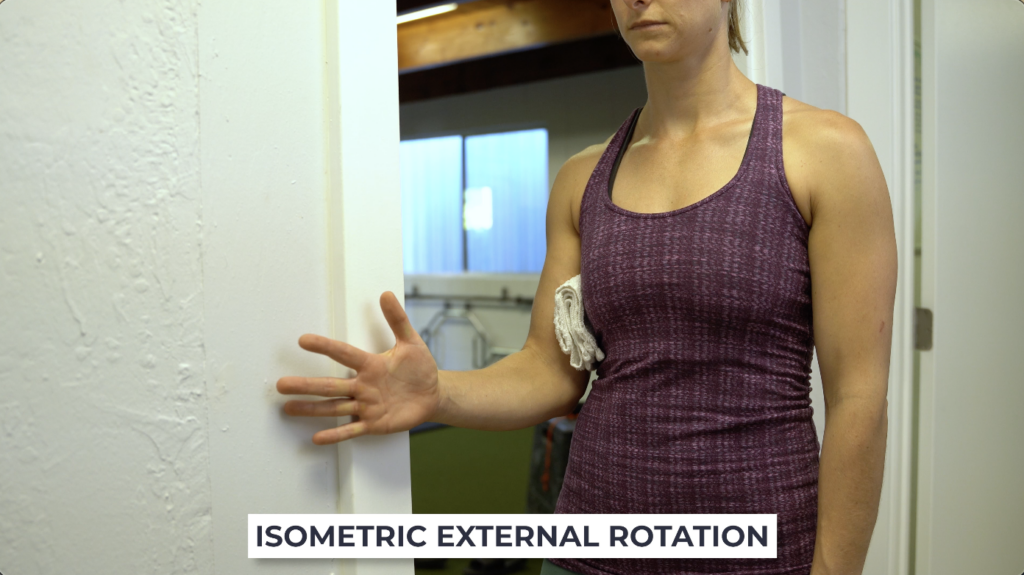
External rotation isometric. The set up will be the same, except now you will press outward against the doorframe or object.
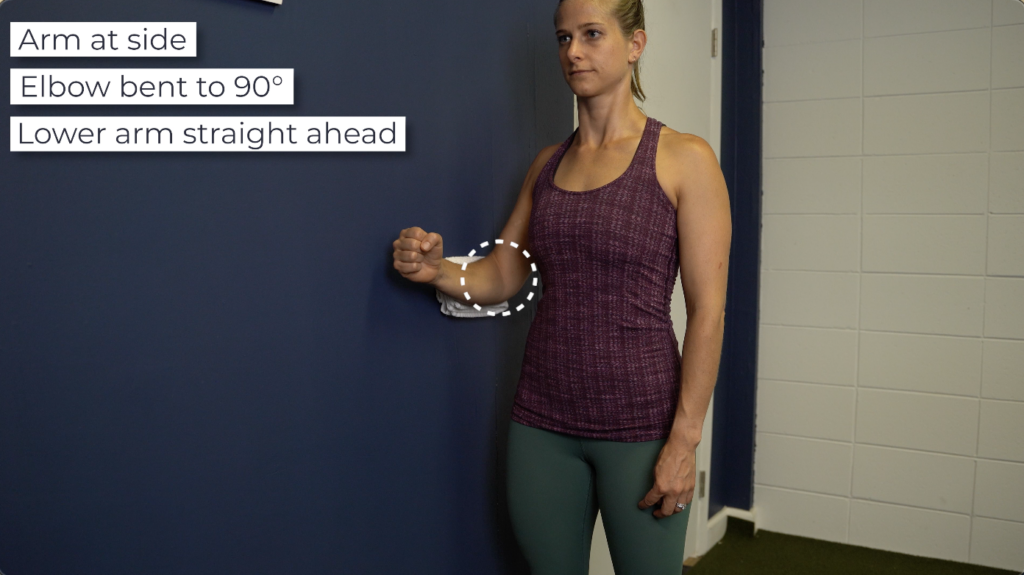
Abduction isometric. Stand with your involved shoulder next to a wall, elbow bent to 90° and lower arm straight ahead. Push your arm away from your body into the wall.
For these, slowly ramp up to the highest intensity possible without pain and hold for a duration of 20-40 seconds. Perform 1-3 sets, 1-2 times a day, everyday, or within tolerance.

Moderate irritability.
Keep pain tolerable during exercise (≤3/10) and make sure you do not have an increase in symptoms the next day. Continue the previous exercises or if tolerated, here are some progressions:
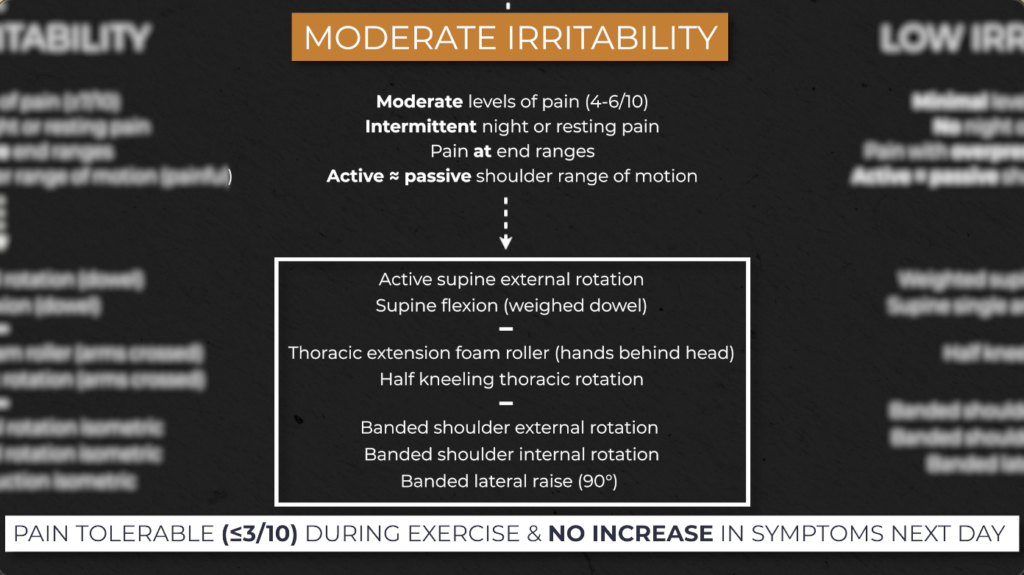
Active supine external rotation. Lie on your back, with your arm supported at your side, and actively rotate your arm outward, keeping your elbow bent to 90°. Move in and out of a tolerable end range.
As your motion improves, perform the same movement but with your arm further away from your body, working up to 90° of shoulder abduction.


Supine shoulder flexion with a weighted dowel. If tolerated, add a weight to the dowel- even as little as 1 lb- and perform the same pullover as previously described. The added weight will help move the shoulder further overhead.

For either of these options, perform for 2-3 sets of 10-15 repetitions, 1-2x a day, everyday or within tolerance.

For thoracic extension and rotation, you will either continue with the same variations mentioned previously, or if tolerated, you will manipulate arm placement.
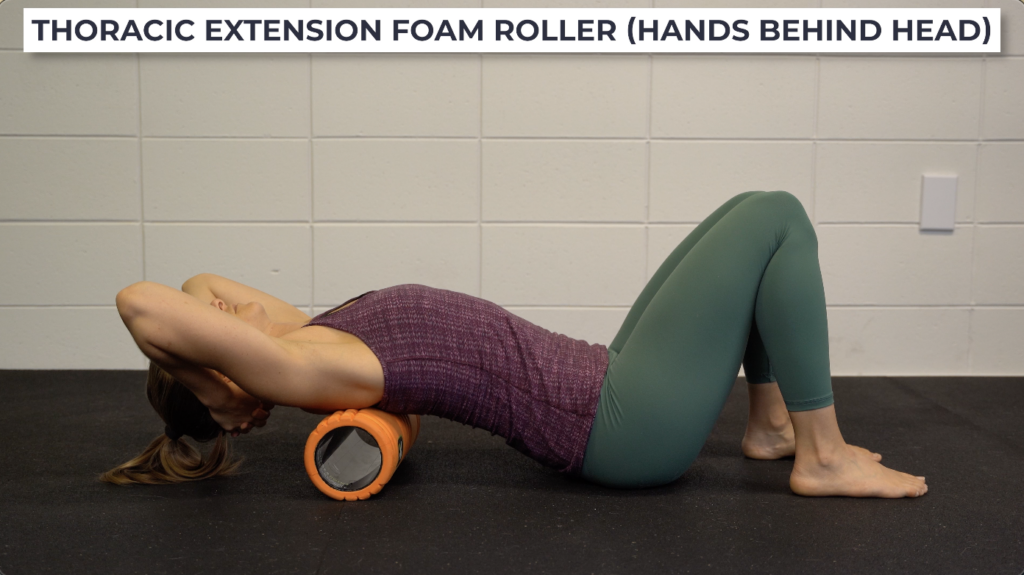
Thoracic extension hands behind head. You will now place both arms behind the head as you move in and out of extension over a foam roller.
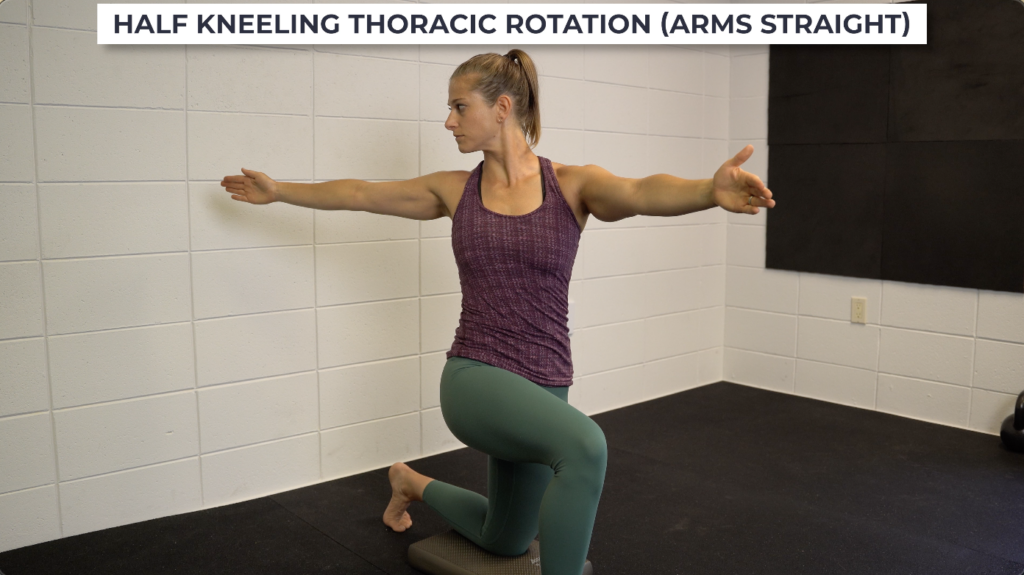
Half kneeling thoracic rotation. You will now keep the arms straight as you rotate, reaching the arm as far back as you can.
Perform for 2-3 sets of 10-12 repetitions, 1-2x a day, every day or within tolerance.

And finally, shoulder strength exercises will progress from isometrics to isotonics, or in other words, moving through your full available range of motion against resistance.
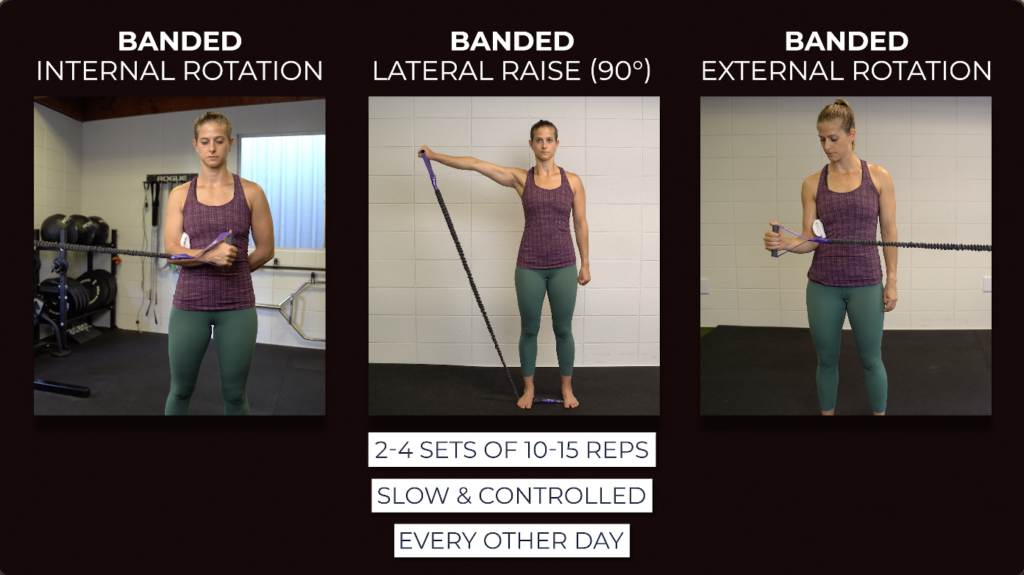
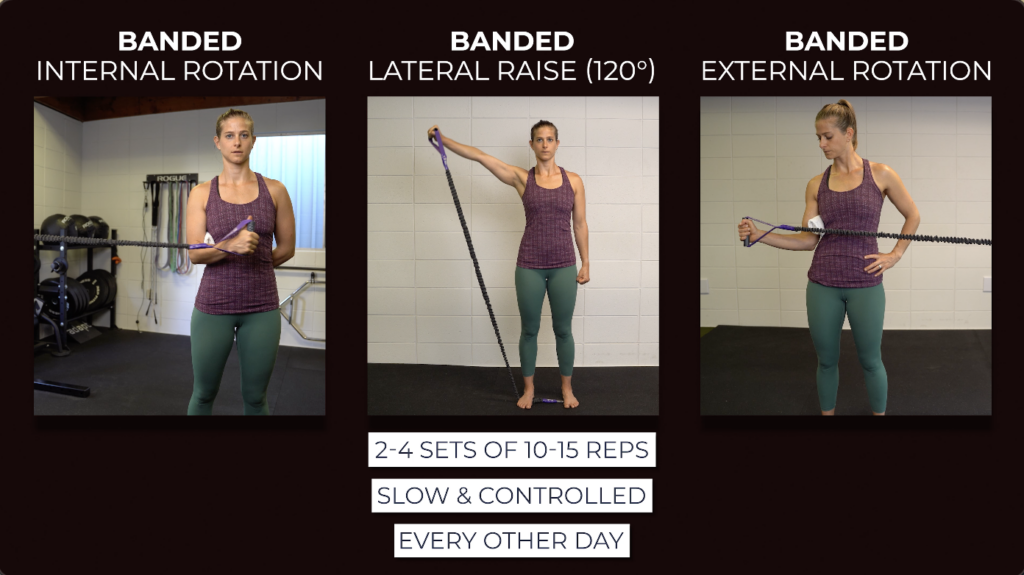
Banded internal rotation. With the elbow bent to 90°, place a towel under the arm to help maintain a neutral shoulder position. Holding a band, rotate inward toward your stomach and then slowly control back to the start.

Banded external rotation. Similar set up but now rotate outward. Throughout the entire motion, try and keep your elbow bent to 90°.

Banded single arm lateral raise to 90°. Stand on a band to anchor it and then raise your arm outward to about shoulder height.

2 suggestions if you find these uncomfortable. First you can lift the arm in scaption. This is not directly at your side or in front of you, but instead the motion is in between. And second you can perform a lateral raise but reduce the range of motion to below shoulder height.

For banded shoulder strength exercises, you will perform 2-4 sets of 10-15 challenging repetitions, at a controlled speed, every other day.
Low irritability
Keep pain tolerable during exercise (≤3/10) and make sure you do not have an increase in symptoms the next day. Continue the previous exercises or if tolerated, here are some progressions:
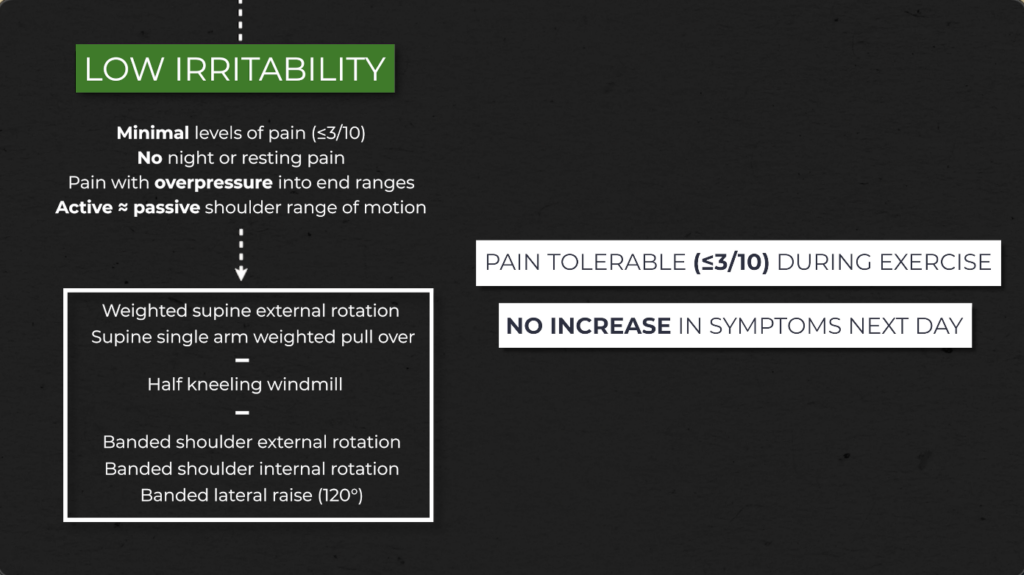
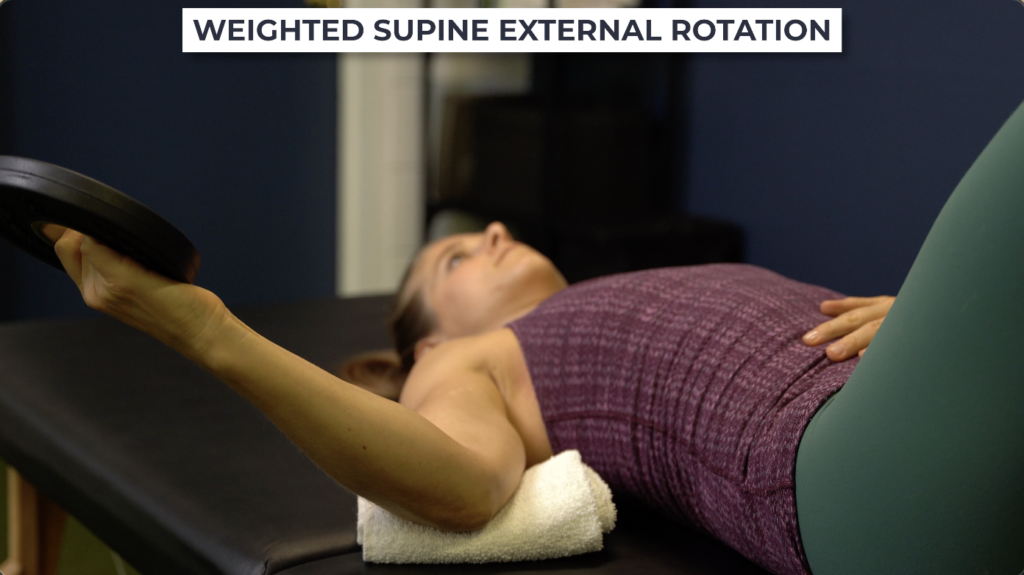
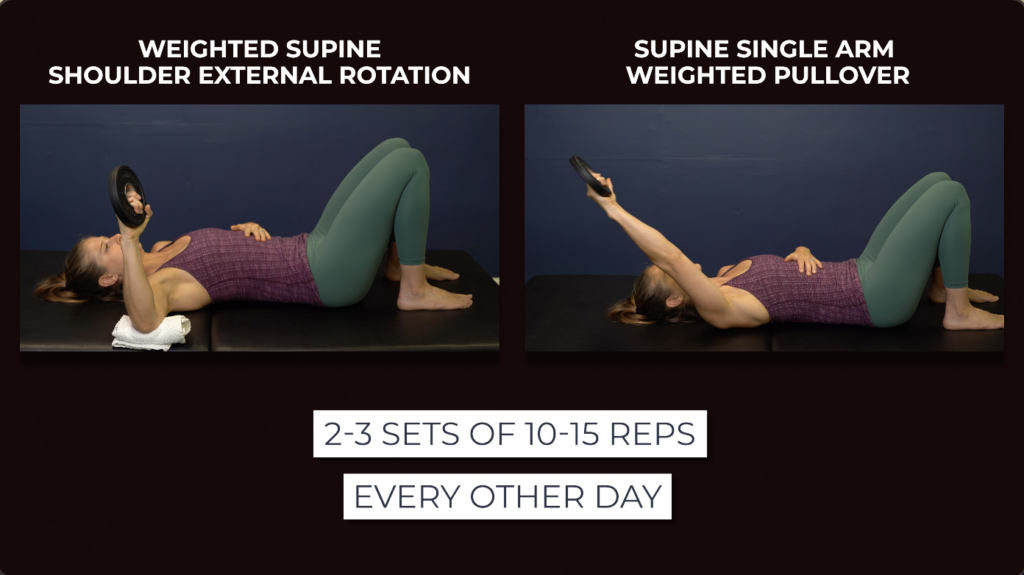
Weighted supine external rotation. Hold a weight, even as little as 1 lb, and rotate your arm outward. Start with your arm at your side, and as your motion improves, move your arm further away from your body, working up to 90° of shoulder abduction.

Weighted single arm pullover. Keep your elbow straight and low back flat to the floor while you pull a weight overhead as far as tolerable. As range of motion improves you can progress by performing on a bench or elevated surface.

Perform these for 2-3 sets of 10-15 repetitions, every other day or as needed.
Half kneeling thoracic windmill. Rotate over the “up” knee, trying to make a big circle with the arm, as you rotate through your spine. Throughout the movement, keep your eyes on the moving hand as this will help maximize thoracic rotation.
Perform 2-3 sets of 10-12 repetitions each side, every other day or as needed.

And for shoulder strengthening exercises, continue with banded internal and external rotation and progress banded lateral raise by increasing range of motion from 90° to 120°, if tolerance allows.
Perform these for 2-4 sets of 10-15 challenging repetitions, at a controlled speed, every other day.
Other Exercises and Lifestyle Factors
In addition to these exercises, regardless of your level of irritability, walking and participating in other forms of tolerable exercise is highly encouraged. For example, if you can tolerate push ups, rows, squats, deadlifts, etc, continue to perform those as programmed.
As well, properly managing other lifestyle factors such as stress, nutrition and sleep are important considerations, since all of these can have a profound impact on symptoms and recovery.
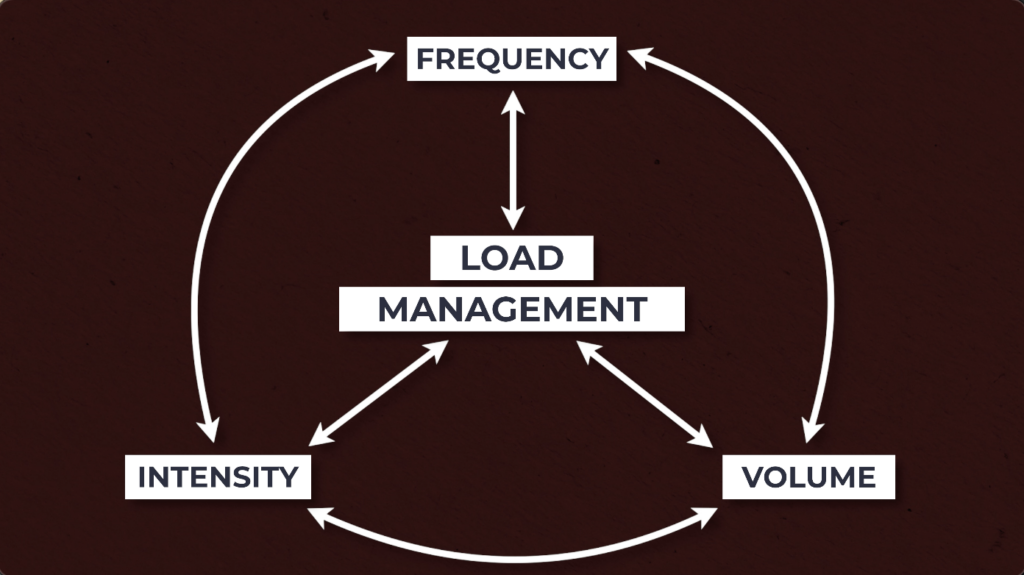
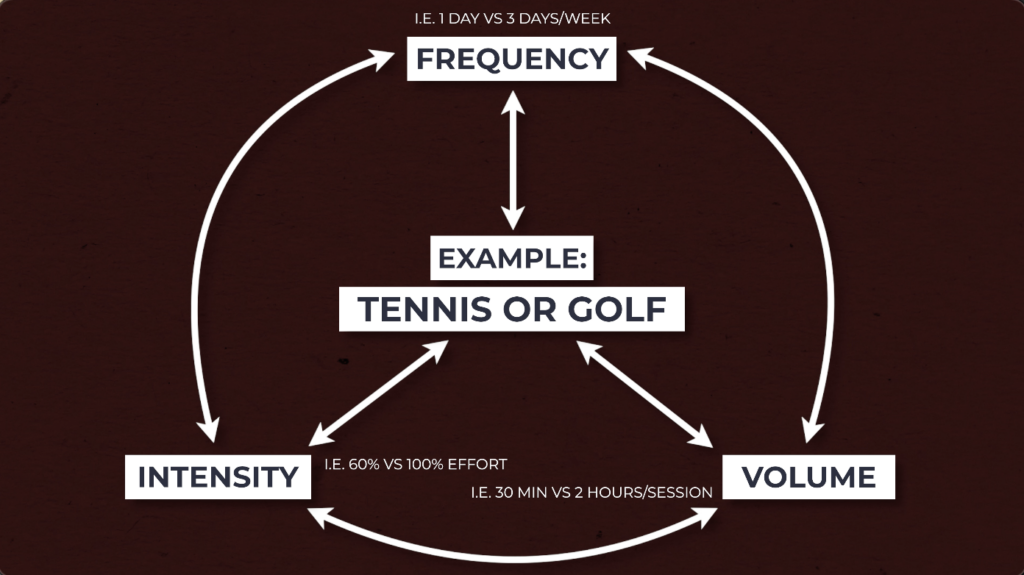
Load Management & Activity Modifications
Consider manipulating the intensity, volume, and or frequency of your desired activity so that you are able to make it more tolerable.
For example, if you enjoy playing tennis or golf, you may need to reduce how often or how much you play.
In some cases, especially higher levels of irritability, you may even need to temporarily stop certain activity and re-introduce it later, as irritability improves. But this does not mean stop everything. You can consider substituting it for other activities, such as biking, running, resistance training, etc.
Other Treatment Options
The UK Frozen Shoulder Trials found that after 12 months, manipulation under anesthesia, arthroscopic capsular release and physiotherapy plus steroid injection all led to superior improvements, but neither of the three were clinically superior.
Challoumas et al. found intra-articular corticosteroid injections to be helpful in the short term when compared to other, non-exercise based treatments. Additionally, a home exercise program was clinically significant compared to no treatment.
A 2019 systematic review compared different pharmacological interventions and found intra articular corticosteroids to provide “clinically meaningful improvements in the short term.”
A study from Cho et al. concluded that steroid injections can be helpful for pain management in the short term, but showed no difference between control groups in the long term.
Kraal et al. 2020 did a scoping review on the pathophysiology of frozen shoulder, and their results help explain “why intra-articular corticosteroid injections should be used early on in the condition and why the intensity of physiotherapy should be guided by tissue irritability.”
And finally, Kelly et al. found corticosteroid injections led to an immediate, significant improvement in shoulder range of motion, implicating “pain and muscle guarding, as opposed to fibrosis or adhesions, as the initial barrier to joint motion.”
Frozen Shoulder Summary
Frozen shoulder will present with shoulder pain and a progressive loss of both active and passive shoulder movement, most notably a loss of passive external rotation greater than 50% of the uninvolved shoulder or less than 30° and deficits in range of motion of greater than 25% in 2 other planes.
While inflammation, capsular thickening and restrictions in adjacent tissues play a role in symptoms and presentation, you also need to strongly consider muscle guarding and pain as major contributors to movement deficits.
This is why choosing exercises and treatment based on your shoulder’s irritability levels can be helpful guidelines to follow.
When irritability is higher, focus on performing relatively pain free shoulder and thoracic range of motion exercises and shoulder isometrics. Since pain may limit activities, strongly consider walking more and implementing strategies to reduce stress. In addition, corticosteroid injections may provide short term benefits since they can help dampen the inflammatory response and reduce pain.
As irritability moves from high to moderate to low, progress exercises by adding weight and increasing the range of motion you move through. Keep pain tolerable during exercise (≤3/10) and make sure you do not have an increase in symptoms the next day.
In addition to these options, you may want to consider other range of motion and strengthening exercises, depending on your restrictions, goals, etc.
And finally, understanding the clinical course of frozen shoulder helps set realistic expectations. The time frame for recovery is extremely variable and not quite as predictable. Pain and function can eventually improve, but this process will take time, effort, and consistency.