The purpose of this blog is to discuss meniscus tears and provide a comprehensive framework for rehabilitation. This includes range of motion, strength, balance, and plyometric exercises.
Looking to improve your strength, range of motion, and power to enhance your function and performance? Check out our Knee Resilience program!
Anatomy & Function
The meniscus is a fibrocartilaginous structure located between the femur, or thigh bone, and tibia, or shin bone. There are 2 in each knee: the medial meniscus located on the inner portion of the knee, and the lateral meniscus located on the outer portion of the knee.
They function to provide shock absorption, force transmission, and stability to the knee joint.

Meniscus Tears
Meniscus tears are either:
- Traumatic, in which there is a distinct mechanism of injury.
- Non-traumatic, which occurs secondary to age-related changes. These are also known as degenerative meniscus tears.
They are often classified according to location and orientation. Tears can be vertical longitudinal, vertical radial, horizontal, oblique, or complex. Vertical or oblique tears that twist and fold over within the joint are termed bucket handle tears (Mordecai et al. 2014)
Previous Beliefs
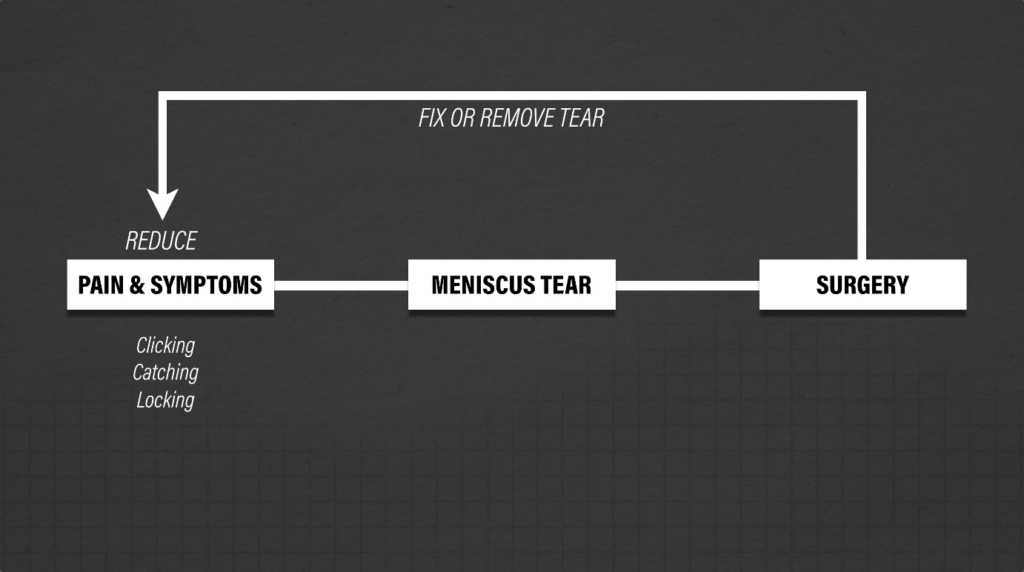
Over the years, the presence of pain and mechanical symptoms, such as clicking, catching, and locking of the knee, were thought to be caused by a meniscus tear. Therefore, in order to reduce symptoms, surgery to repair or remove the meniscus was performed.
Dispelling Myths
However, the current scientific literature does not fully support this theory. Here are 3 things you should know:
1. There is not a simple cause and effect relationship between symptoms and meniscus tears.
For example, Thorlund et al. 2018 found that these “mechanical symptoms were equally prevalent in patients with and without a meniscal tear,” and are actually common in “those with knee problems in general.”
Other research by Pihl et al. 2018 concluded that these symptoms have “limited utility as an indicator for the presence of meniscal tears”, and McHugh et al. 2022 found that “mechanical symptoms are not useful clues to the diagnosis of symptomatic meniscal tears.”
2. Meniscus tears are common in asymptomatic individuals.
Horga et al. 2020 found that in 230 uninjured knees, 97% of knees showed MRI abnormalities, with 30% having meniscal tears. They went on to conclude: “Our study questions the clinical decision-making regarding arthroscopy and its efficacy in reducing symptoms and treatment.”
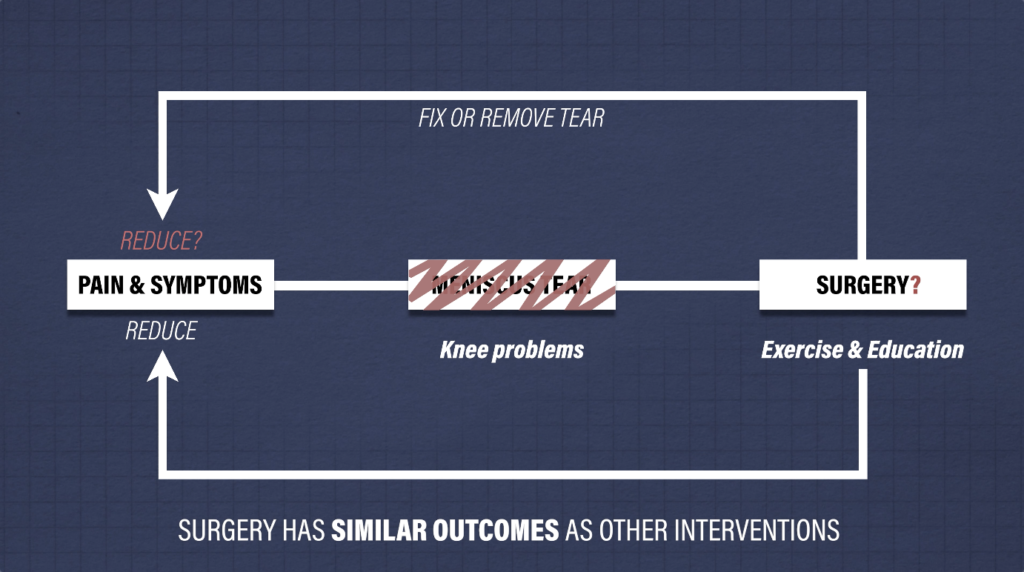
3. Surgery to remove or repair the meniscus has not been shown to lead to better outcomes compared to other interventions.
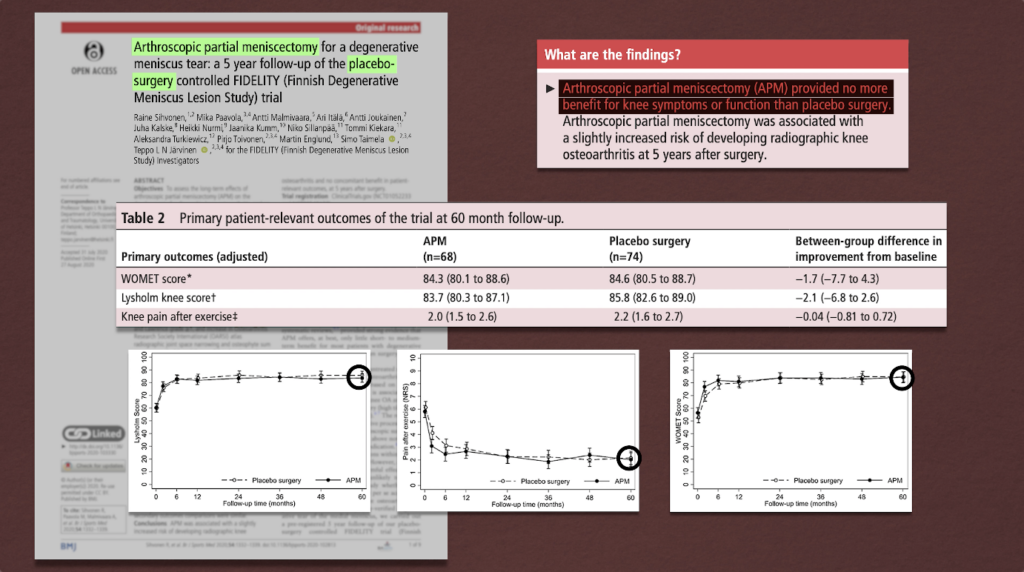
For example, Sihvonen et al. 2020 compared a partial meniscectomy, a surgery where part of the meniscus is removed, to a placebo or sham surgery. Over the course of 5 years, surgery “provided no more benefit for knee symptoms or function than placebo surgery.” It even led to an “increased risk of developing radiographic knee osteoarthritis.”
In fact, a 2022 Cochrane Review concluded that arthroscopic surgery for degenerative meniscal tears “provides little or no clinically important benefit in pain or function, probably does not provide clinically important benefits in knee-specific quality of life, and may not improve treatment success compared with a placebo procedure.”
Most studies to date have exclusively looked at surgical outcomes in an older population with degenerative meniscus tears – “older” being those over the age of 40.
But an observational study by Pihl et al. 2018 did find that “younger patients under 40 years old with mechanical symptoms did have greater improvements after surgery compared to those without symptoms.” However, the authors did go on to say that “randomized controlled trials are still needed to confirm this potential benefit.”
Takeaway: This information means that if you have knee symptoms related to a degenerative meniscus tear, surgery is likely not indicated. For traumatic injuries in a younger population, research is not as definitive. But the good news is that exercise has been shown to be just as effective in the long term for both populations.
A study by Skou et al. 2022 showed that exercise led to similar improvements in pain, function, and quality of life after 12 months in a younger population with mostly traumatic tears.
And a different study by Kise et al. 2016 showed no clinically relevant difference in knee function after 2 years in an older population with degenerative tears.
For degenerative meniscus tears, current clinical practice guidelines favor conservative management and even “recommend against arthroscopic knee surgery.”
Meniscus Tears Exercise Overview
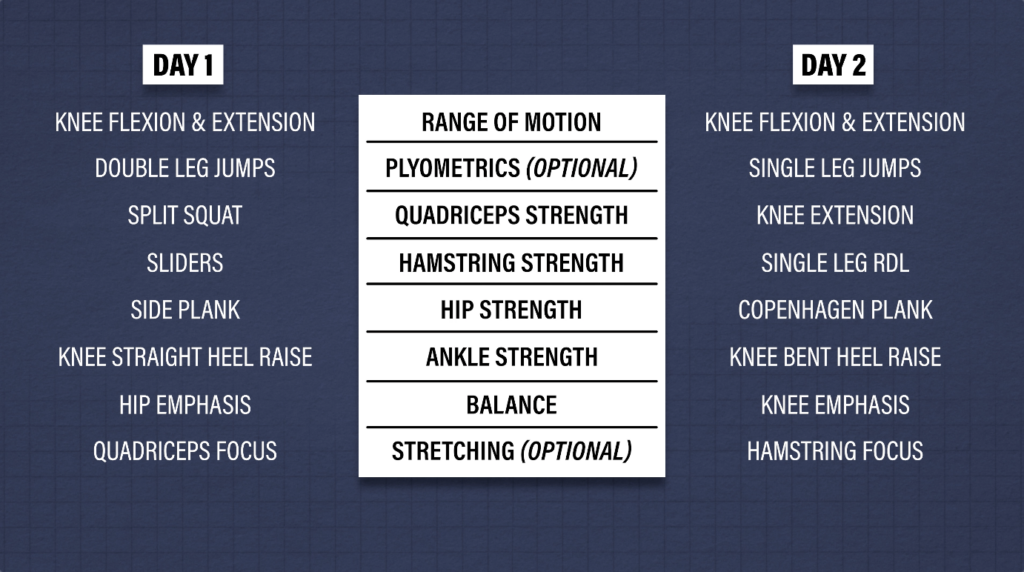
For the exercises, I am going to present a comprehensive rehab program that covers multiple categories aimed at increasing your capacity and tolerance to various stressors. Within each category, I will provide multiple exercise options, ultimately giving you two different workouts to follow.
Disclaimer: These exercises are intended for non surgical cases. If you had surgery, you will ultimately follow a similar framework, but before starting exercises, talk to your doctor or Physical Therapist as you may have weight bearing precautions or other restrictions to consider.
Category 1: Knee Range of Motion
Ideally, you should be able to fully straighten your knee and touch your heel to your butt. At minimum, you should aim to restore extension and flexion that is equal to your uninjured side.

For knee extension, or straightening, here are 3 options:
1. Seated active quad contractions. Straighten your leg and squeeze your quad for 10 seconds. Repeat this for 10 repetitions, 3 times a day, every day. If your motion is improving, you can use a towel or strap to pull up on your foot in order to intensify the stretch.

2. Heel prop. Prop your heel up on an elevated surface for 10 to 15 minutes, three times a day, every day. If you need to enhance the stretch, you can add a weight just above your knee. The goal here is low load, long duration, so while it may feel slightly uncomfortable, it should not be unbearable.

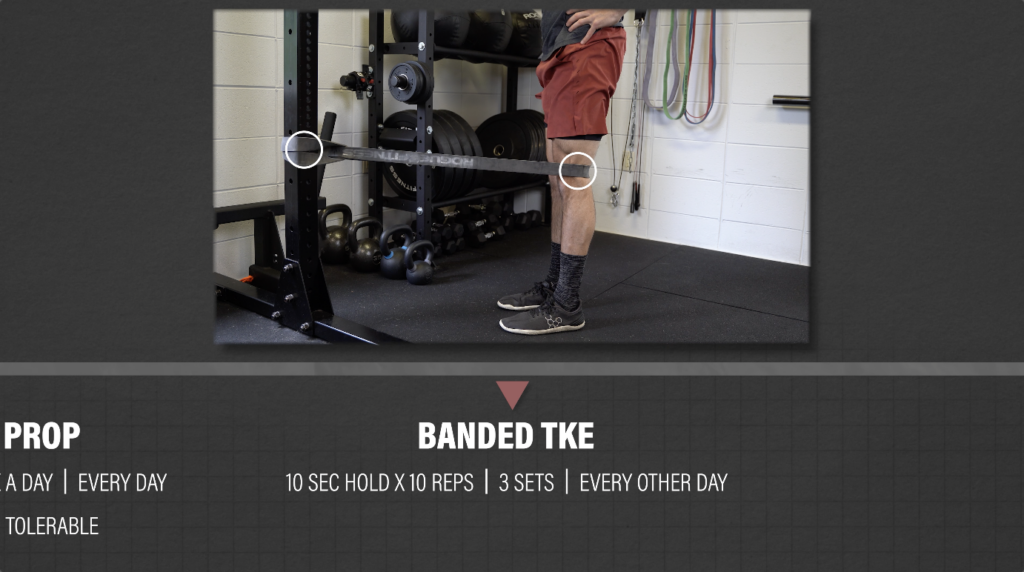
3. Banded TKE. Once you gain more range of motion, strength, and control, add in a banded TKE. Place a band behind the back of your knee, anchored to an object and perform the same quad contractions against resistance. Perform for 3 sets of 10 reps (10 second hold each rep), every other day.
For knee flexion, or bending, here are 3 options:
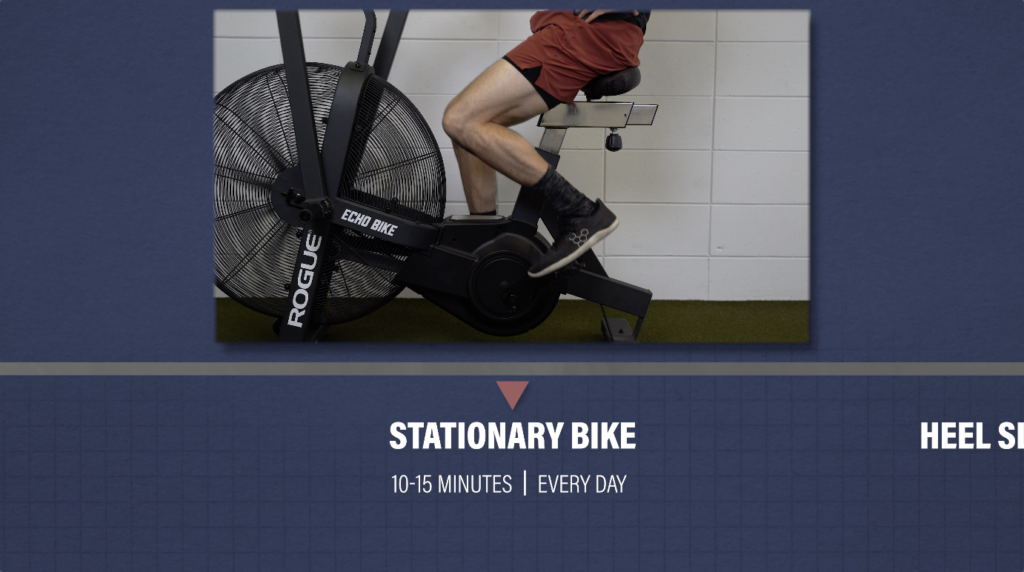
1. Stationary bike. Start with the seat at a higher level, and as range of motion improves, lower the seat to expose the knee to more flexion. Perform for 10-15 minutes, every day.
2. Heel slides. You can use a slider on carpet or a towel on a hard surface. Start by actively sliding your heel toward your butt. As motion improves, progress by using a towel or strap to pull the knee into more flexion. Perform for 3 sets of 10-15 repetitions, 3 times a day, every day.

3. Rock backs. You can perform a quadruped rock back (easier) or tall kneeling rock back (harder). I recommend kneeling on a pad or pillow for these, and you can even experiment with using a towel behind the knee. Anecdotally, I have found this to help patients move into more knee flexion with less discomfort. Perform for 10-15 reps, 2-3x/day, every day.

Category 2: Hip, Knee, and Ankle Strength
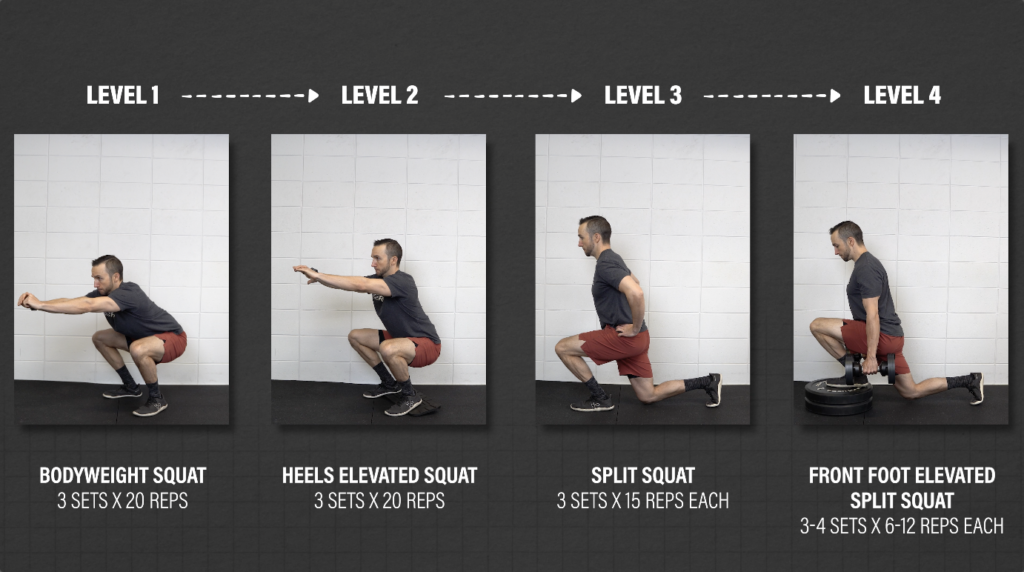
Quadriceps Focus #1: Split squat progression. This will help increase your tolerance to weight bearing knee flexion in deeper positions.
Level 1: Bodyweight squat. Your goal is to perform 3 sets of 20 repetitions, getting your hips to at least parallel. If you need, start with hand assistance, such as using a TRX or another object.
Level 2: Heels elevated squat. Elevate your heels 2-3 inches. This will help keep your torso more upright and allow you to go deeper, moving your knee into more flexion. Your goal is 3 sets of 20 repetitions, and again, try to get your hips to at least parallel.
Level 3: Split Squat. Stand in a split stance and lower down while driving the front knee forward as far as you can. Your goal is 3 sets of 15 controlled reps on each leg before progressing.
Level 4: Front foot elevated split squat. Elevate the front foot on an object 2 to 4 inches high and lower down, driving the front knee forward. Perform for 3-4 sets of 6-12 reps each leg. Overtime, you can increase depth and add weight.
Quadriceps Focus #2: Single leg knee extension.
Your goal is to move through the full range of motion with weight at a challenging intensity, but to start, you can shorten the range of motion or even perform with no weight, if needed. Perform for 3-4 sets of 10-15 reps on each leg.

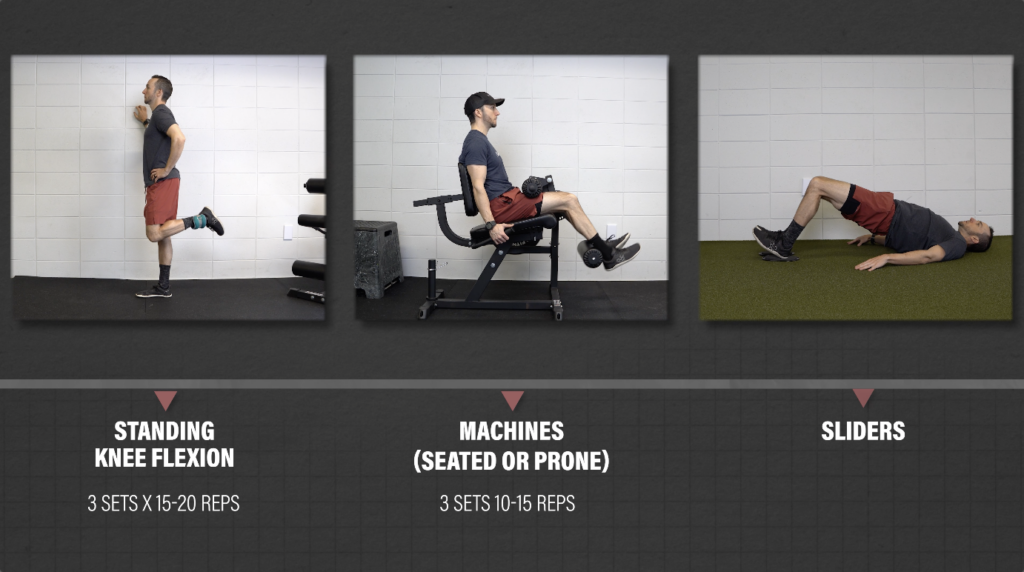
Hamstring Focus #1: Knee Flexion.
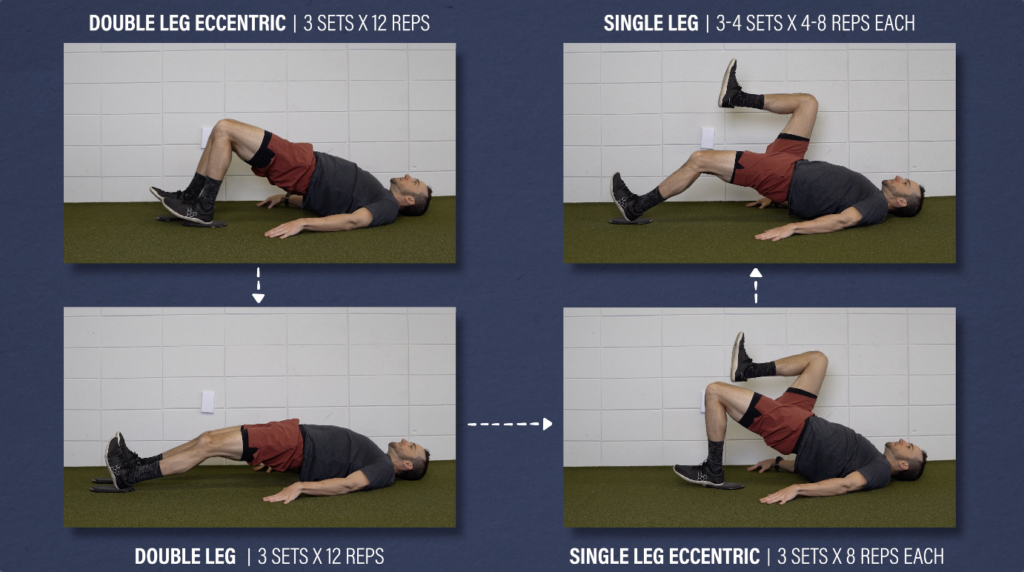
You can perform standing knee flexion with an ankle weight, use machines, or an exercise I like to use: hamstring sliders.
Level 1: Double leg eccentric sliders. Bridge up and slowly straighten your legs. Lower down and repeat. Build up to moving through your full range of motion for 3 sets of 12 reps.
Level 2: Double leg sliders. Keep your hips up the whole time for 3 sets of 12 reps.
Level 3: Single leg eccentric sliders for 3 sets of 8 reps each leg. (3×8 reps
Level 4: Single leg sliders for 3-4 sets of 4-8 reps each.
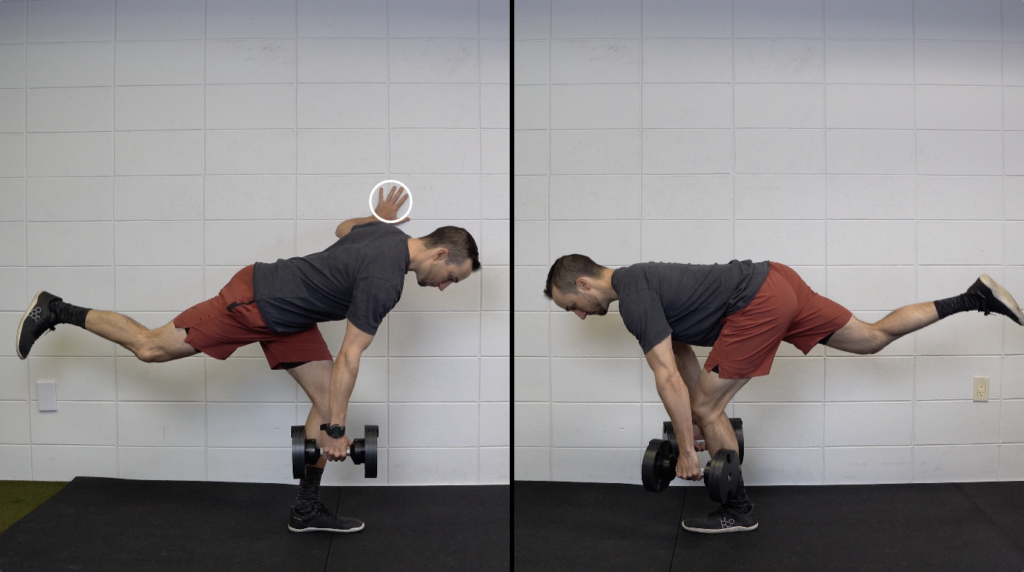
Hamstring Focus #2: Weighted single leg RDL.
This option focuses on targeting the hamstrings through hip extension. Keep a slight bend in the knee and hinge in your hips, lowering until your chest is about parallel to the ground.
If you struggle with balance, you can do these with a hand supported on a wall or object, but ultimately, your goal should be to do these without upper body assistance. Perform for 3-4 sets of 8-12 reps on each leg.
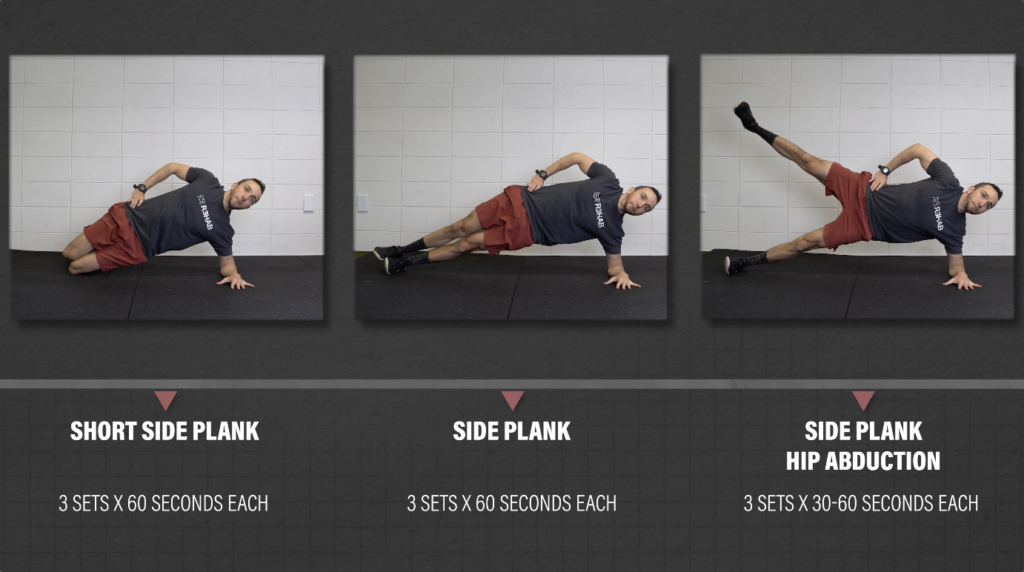
Hip Focus #1: Lateral Hip (Abductors)
Level 1: Short side plank isometric for 3 sets of 30 seconds each side.
Level 2: Long side plank isometric for 3 sets of 30 seconds each side.
Level 3: Side plank with hip abduction for 3 sets of 30-60 seconds each. Slowly lift and lower the top leg under control.
Hip Focus #2: Medial Hip (Adductors)
Level 1: Supine ball squeeze isometric. Lie on your back and place a ball or pillow between your ankles. Squeeze as hard as you can, keeping pain to a tolerable level. Your goal is to build up to a maximum effort squeeze for 3 sets of 30 seconds.
Level 2: Short Copenhagen plank isometric for 3 sets of 30 seconds each side.
Level 3: Long Copenhagen plank isometric for 3 sets of 30-60 seconds each side.
Level 4: Long Copenhagen plank. Lower and lift your bottom hip and leg under control for 3-4 sets of 6-12 reps on each side.

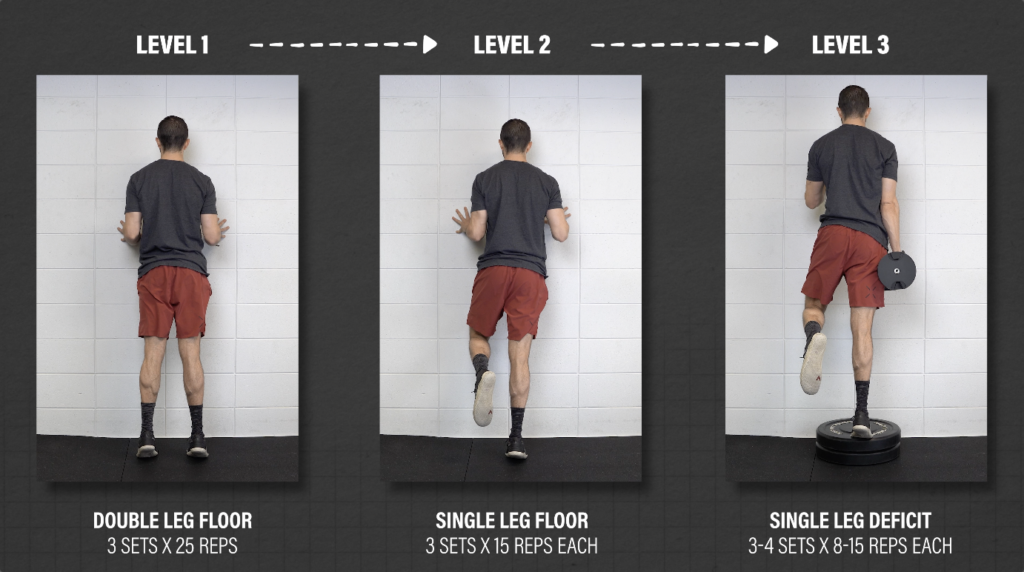
Ankle Focus #1: Knee Straight Heel Raise
Level 1: Double leg heel raises from the floor for 3 sets of 25 reps.
Level 2: Single leg heel raise for 3 sets of 15 reps on each leg.
Level 3: Deficit single leg heel raise for 3-4 sets of 8-15 reps each leg. To make these harder, add weight over time.
Ankle Focus #2: Knee Bent Heel Raise
The other calf option is performing a knee bent variation. I personally like the seated deficit heel raise. Start with your toes on an object about 2-4 inches high and place a weight on top of your knees. You can use a barbell, dumbbells, kettlebells, etc.
To make this easier, you can perform these on the ground or use less weight, but the deficit is a good goal to build up to. Perform for 3-4 sets of 8-15 reps.

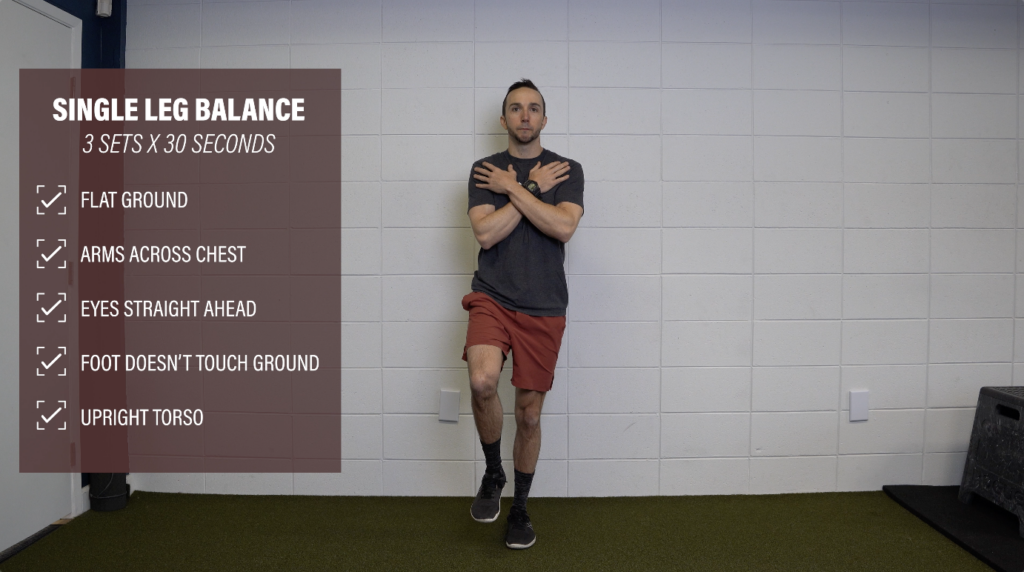
Category 3: Balance/Proprioception
Start by standing on one leg on flat ground with hands across your chest and eyes straight ahead. Don’t let your leg touch the ground or your standing leg, and keep your torso upright. Once you can complete 3 sets of 30 seconds, here are 2 dynamic options to try.
Balance #1: Hip Emphasis
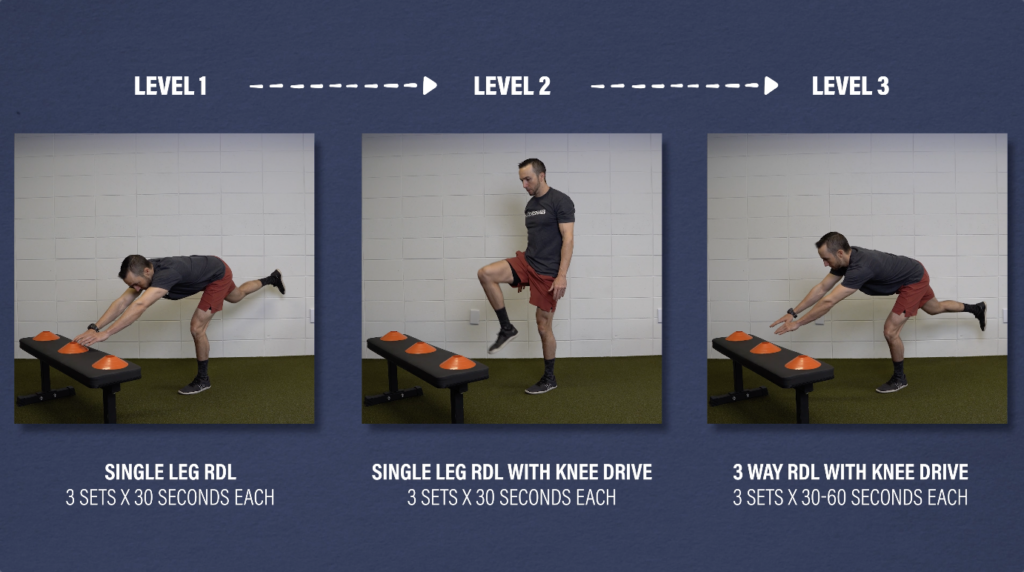
The first is a single leg RDL progression which places an emphasis on moving predominantly through the hips.
Level 1: Single leg RDL for 3 sets of 30 seconds on each leg. If needed, move through less range of motion, but your goal is to eventually get your torso about parallel to the floor.
Level 2: Single leg RDL with knee drive for 3 sets of 30 seconds on each leg.
Level 3: 3 way RDL with knee drive. Reach your arms to the left, middle, and then to the right. Perform for 3 sets of 30-60 seconds on each leg.
Balance #2: Knee Emphasis
The second option is the Y balance. You still move through the hips, but it places slightly more emphasis on loading through the knee.Stand on one leg and reach out in three different directions with the opposite leg, creating a Y shape. Your goal is to reach as far as you can and then return to the starting position without losing balance. Start with smaller reaches and increase the distance over time. Perform for 3 sets of 30-60 seconds on each leg.

Category 4: Optional Stretching
You can add in various stretches if you’re looking to further increase knee range of motion or simply because you find that it feels good.
One option is the couch stretch. Start in a half kneeling position and elevate your back foot on a bench or chair. Tuck your pelvis and lean back toward your heel. You can hold this for time or move in and out of this position. Perform for 2-3 sets of 30-90 seconds on each side.
Another option is alternating knee extension. Place your hands flat on the floor or on an elevated surface. Gently, bend one knee while keeping the other straight. Hold for a second or two and then alternate between legs for 2-3 sets of 30-90 seconds on each side.


Category 5: Optional Plyometrics
If you intend to run, play sports, or are looking to improve your tolerance to jumping and landing, then you should include plyometrics. Ideally, perform these prior to strength exercises. Here are 2 examples:
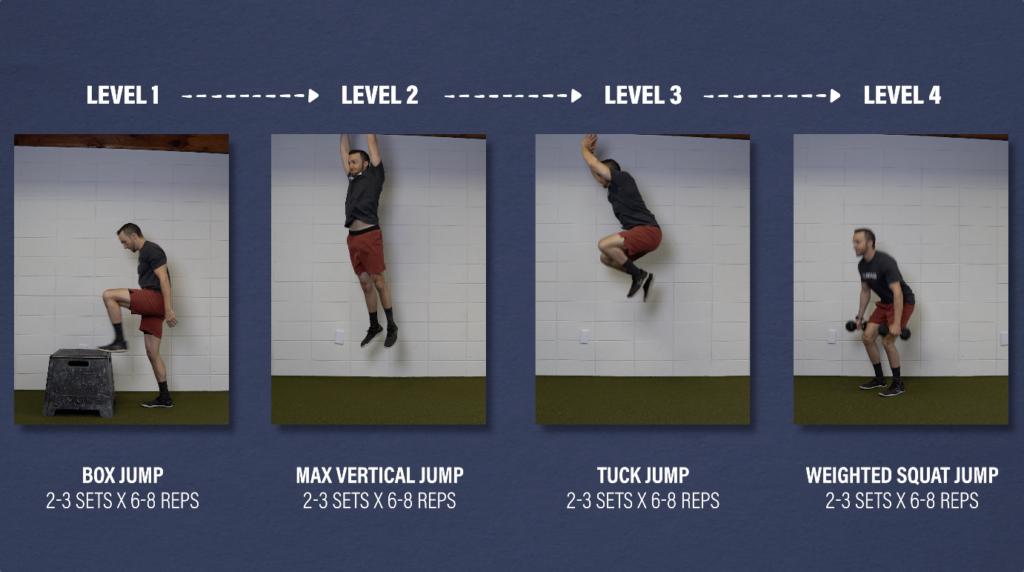
The first option is a bilateral squat jump progression:
Level 1: Box jump.
Level 2: Maximal vertical jump.
Level 3: Tuck jump.
Level 4: Weighted squat jump.
Your focus is on maximal effort each jump,so you are only performing 2-3 sets of 6-8 reps.
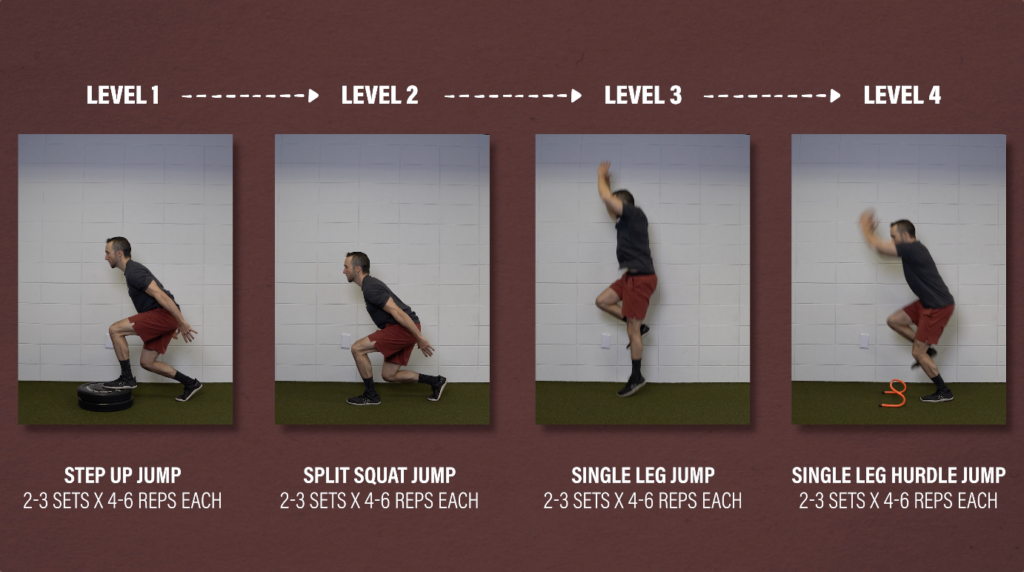
The second option is a single leg jump progression:
Level 1: Step up jump.
Level 2: Split squat jump.
Level 3: Single leg jump.
Level 4: Single leg forward jump over hurdles.
Again, place an emphasis on maximal effort each jump, aiming to perform 2-3 sets of 4-6 jumps on each leg.
Additional Exercise Considerations
As you can see, there are a lot of exercise options, but don’t feel like you have to do all of them. For example, if the couch stretch or kneeling is not tolerable or doesn’t meet your goals, you don’t need to do them.
Also, all of these categories can be performed simultaneously and progressed independently of one another. For example, you may still be working on regaining full knee flexion, but are able to progress to the weighted single leg deficit heel raises.
Programming for Meniscus Tears
In the early stages, focus on improving knee extension and flexion, such as the heel prop and heel slides. Do these often, so multiple times a day, every day
If you are looking for a minimal program, at the very least, you should place an emphasis on improving range of motion and increasing tolerance to weight bearing knee flexion, such as performing a squat or split squat variation.
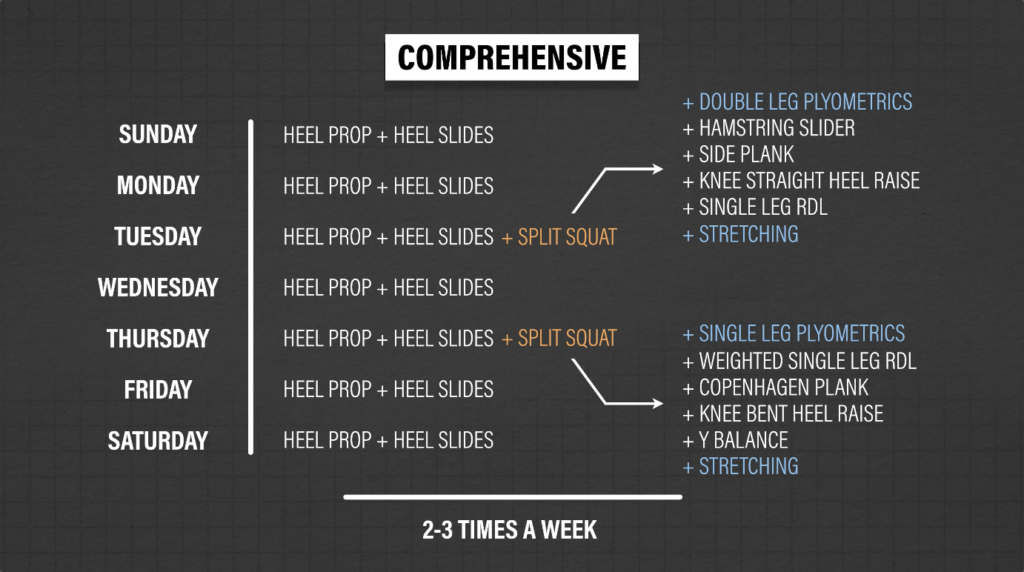
However, my recommendation would be taking a comprehensive approach, which covers the previous options, but also includes other strength and balance exercises. Additional considerations include optional stretches and plyometrics, depending on your needs and goals.
Perform this rehab plan 2-3x/week and keep pain tolerable during exercise.
Return to Sport/Running
If your goal is to return to running or playing a certain sport, the plyometric exercises will help you develop some qualities applicable to these activities. But you will also need to consider sport specific drills, such as cutting and change of directions, as well as gradually returning back to your preferred activity. This process will likely take several months in order to appropriately build up your volume and tolerance.
Summary
Knee pain and mechanical symptoms are quite common in those with knee problems in general, and not specific to meniscus tears.
Even if a tear is confirmed, we cannot say with 100% certainty that symptoms are caused by this finding.
This brings into question the efficacy of surgery. It may be indicated in some cases, but conservative management is currently recommended as the first line of treatment for knee symptoms related to degenerative meniscal tears, and can be an effective option for younger populations with traumatic tears as well.
At the very least, you should place an emphasis on improving knee extension and flexion range of motion, and increasing tolerance to weight bearing knee flexion.
However, a comprehensive approach which includes other strength and balance exercises are strongly recommended. Depending on your needs and goals, you may choose to add in stretching and plyometrics.
Again, these exercises and progressions are just some options to follow. Not everyone will need to include plyometrics or progress to the highest level of each exercise. Build up to the level that is most appropriate for you and your goals.