The purpose of this blog is to discuss lumbar spondylolisthesis and provide a comprehensive framework for rehab, including exercise progressions with sets and reps.
Do you have new, lingering, or recurring low back pain that’s stopping you from doing the things you enjoy or keeping you from feeling like yourself? Check out our Low Back Resilience Program!
Spondylolisthesis
The first half of the word refers to the vertebrae of the spine, while the second half refers to slipping. Therefore, spondylolisthesis is the slipping of one vertebra in reference to the one below it.
The degree of slippage is usually graded using the Meyerding Classification System based on x-rays in standing.
- Grade 0: No slip
- Gade I: 1% to 25%
- Grade II: 26% to 50%
- Grade III: 51% to 75%
- Grade IV: 76% to 100%
- Grade V: Complete slippage
Of those with spondylolisthesis, grade 1 is most common.
There are also various classifications systems to describe the types of spondylolisthesis. In 1976, Wiltse, Newman, and Mcnab presented 5 categories:
- Dysplastic, which is a congenital condition.
- Isthmic, which most commonly occurs at L5-S1 and affects younger individuals, is associated with stress fractures of the pars interarticularis. This specific type of fracture is known as a spondylolysis.
- Degenerative, which most commonly occurs at L4-L5, is associated with age-related changes of the spine.
- Post Traumatic
- Pathologic
Isthmic and degenerative spondylolisthesis are the focus of this blog.
Exercise Rationale
If spondylolisthesis is related to structural changes of your spine, how can exercises help? Why not jump straight to surgery and correct the issue?
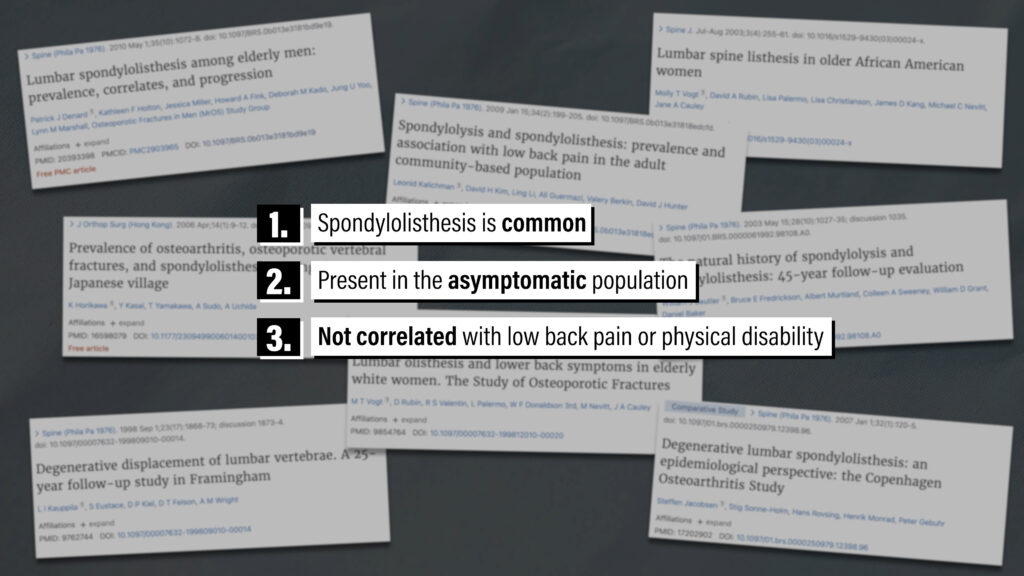
Well, research suggests that spondylolisthesis is common, present in the asymptomatic population, and is not correlated with low back pain or physical disability (Denard 2010, Kalichman 2009, Jacobsen 2007, Horikawa 2006, Vogt 2003, Beutler 2003, Vogt 1998, Kauppila 1998). For example, Kalichman et al in 2009 found that in their participants of men and women between the ages of 40 and 80, 11.5% had spondylolysis, 8.2% had isthmic spondylolisthesis, and 13.6% had degenerative spondylolisthesis. The authors concluded that “no significant association was identified between spondylolysis, isthmic spondylolisthesis, or degenerative spondylolisthesis, and the occurrence of low back pain.”
Therefore, the purpose of exercise isn’t to change the structure of your spine on imaging. The goal is to gradually improve your function and quality of life.
The exercises that I’m going to present should be considered along a continuum. On one end, exercises will require minimal to no lumbar spine range of motion, lower relative loads, and no speed component. An example of an exercise like this would be a plank. On the other end, exercises will require more range of motion, higher relative loads, and may have a speed component. Examples include medicine ball throws and heavy deadlifts.
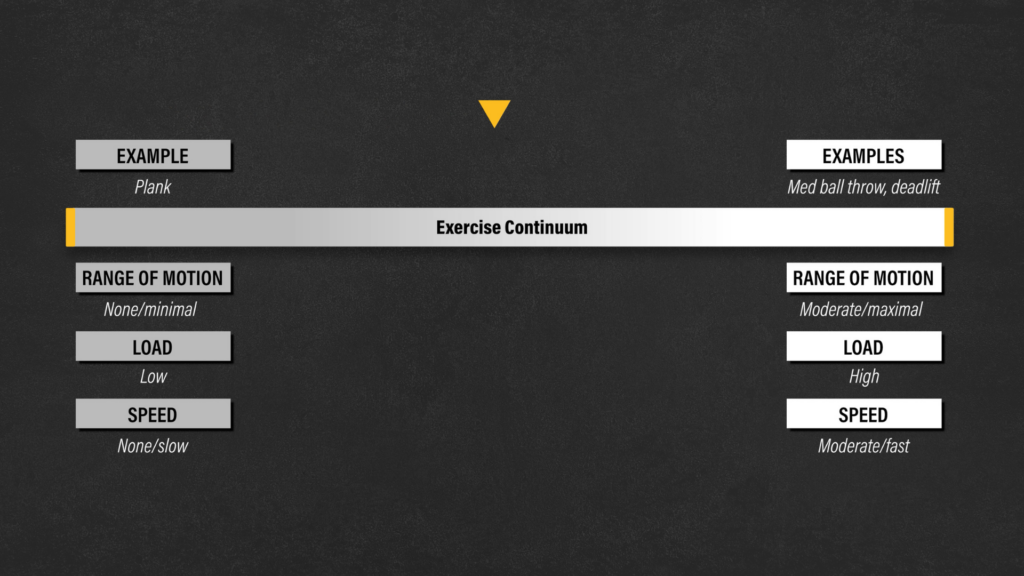
If your goal is to simply improve your walking tolerance, you might stay on the left side of the continuum. However, if you want to return to overhead sports, gymnastics, or powerlifting, you’ll likely have to work toward the right side of the continuum.
(Anti) Extension
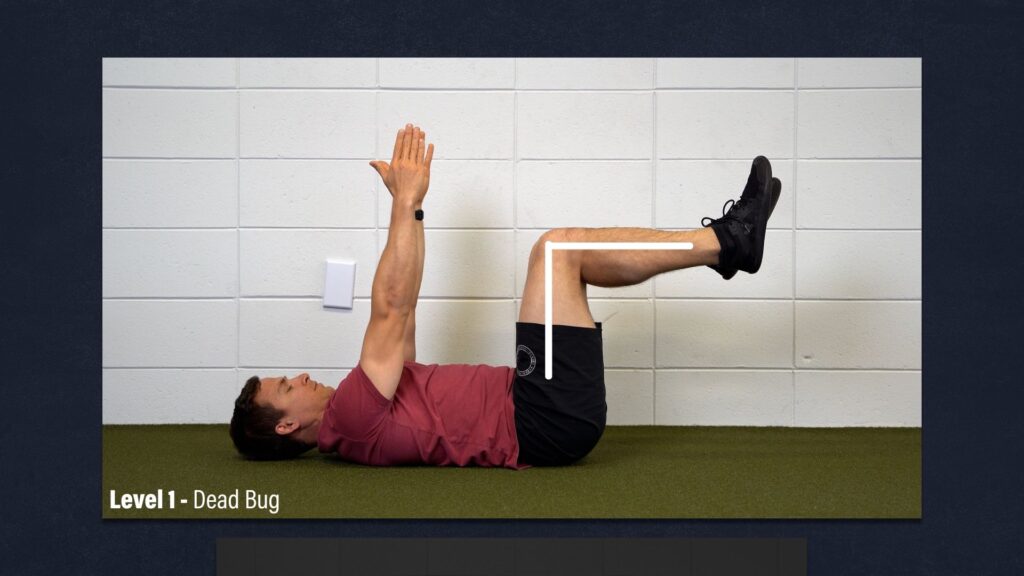
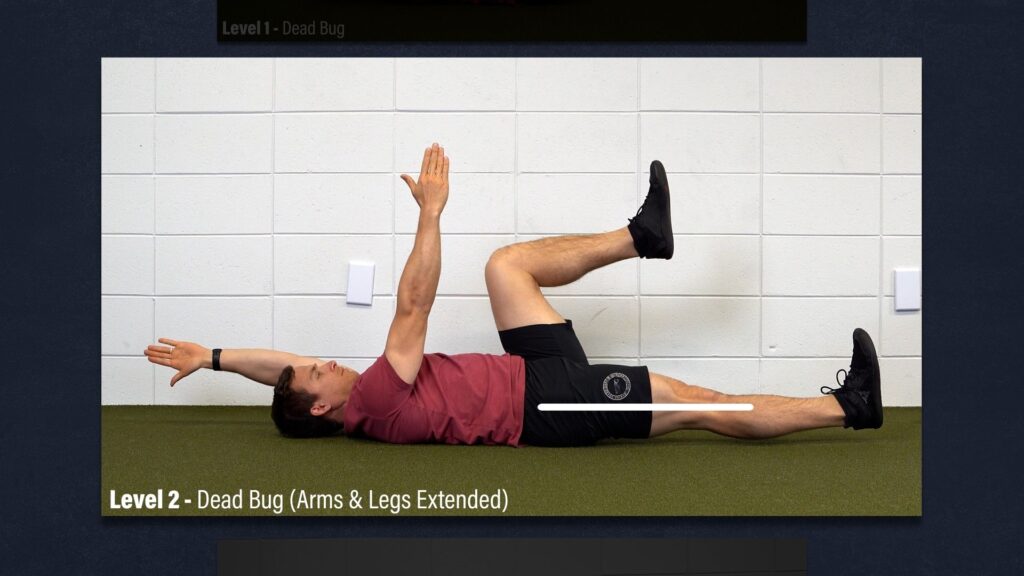
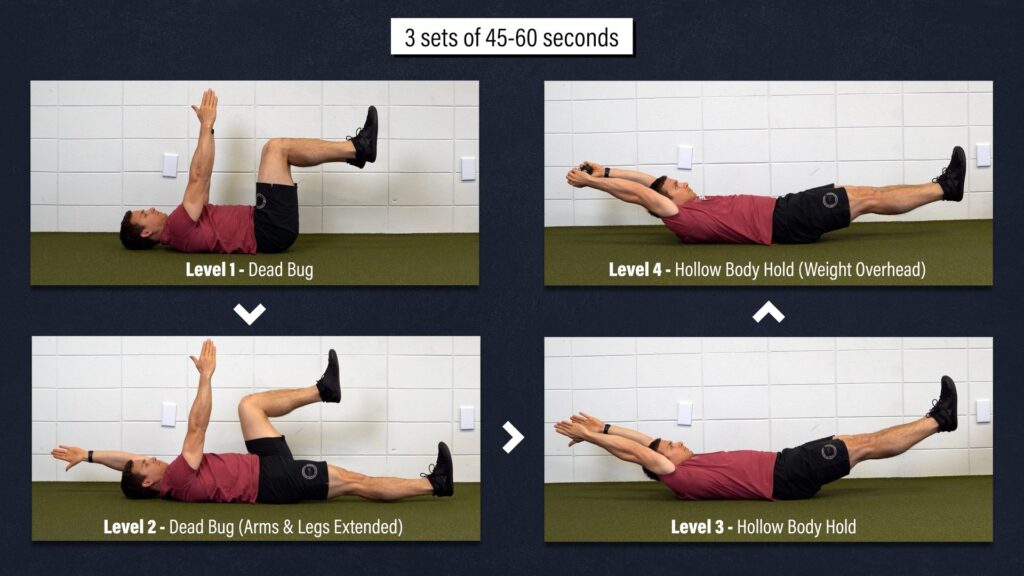
Level 1 – Dead Bug. Start on your back with your hips and knees bent to 90 degrees and your arms straight out in front of you. Flatten your low back into the floor to engage your abs and hold this position. If this is too difficult, rest your arms by your side.
Level 2 – Dead Bug w/ Extended Arms & Legs. Reach one arm overhead, straighten the opposite leg, and hold this position for half of the prescribed time before switching sides. If this is too challenging, you can bring your arms and legs closer to midline.
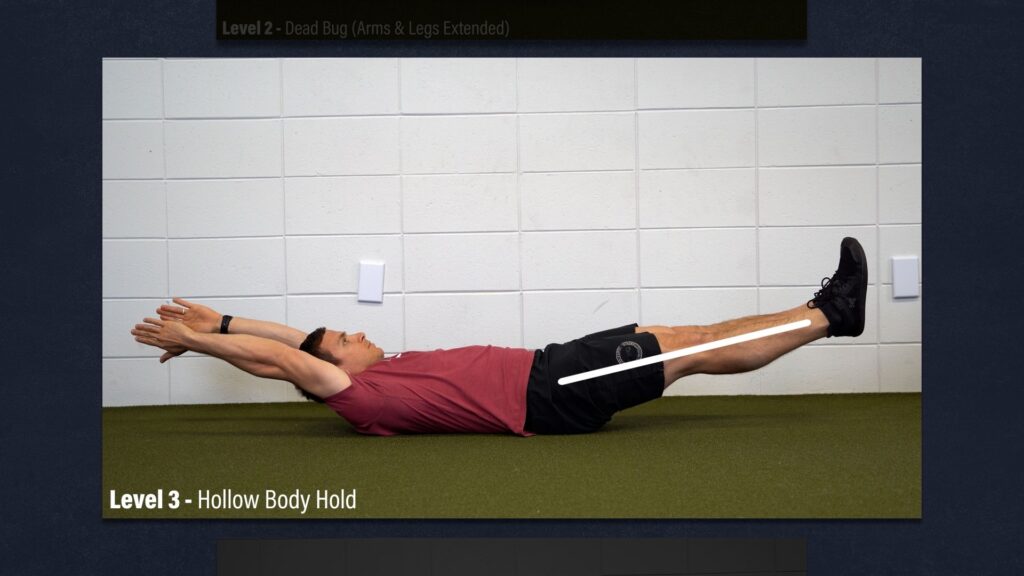
Level 3 – Hollow Body Hold. With your arms overhead and legs straight, lift your legs, shoulders, and head off the ground. Keep your low back flat and abs engaged as you imagine yourself forming the shape of a banana. Once again, you can bring your arms and legs closer to midline if this is too difficult.
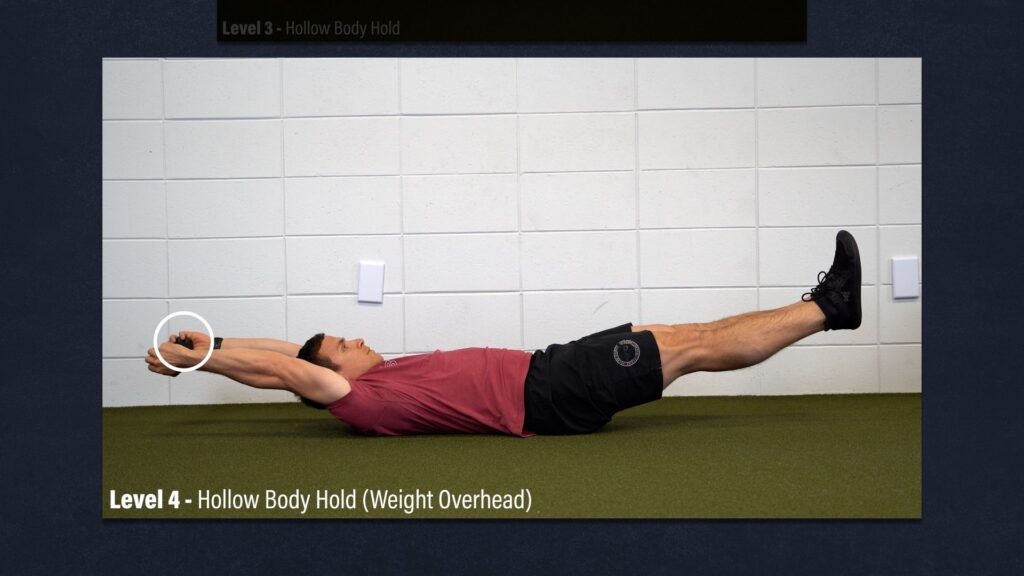
Level 4 – Hollow Body Hold w/ Weight Overhead. Progressively add weight to the exercise to make it more challenging.
Aim for 3 sets of 45-60 seconds as you work through each exercise.
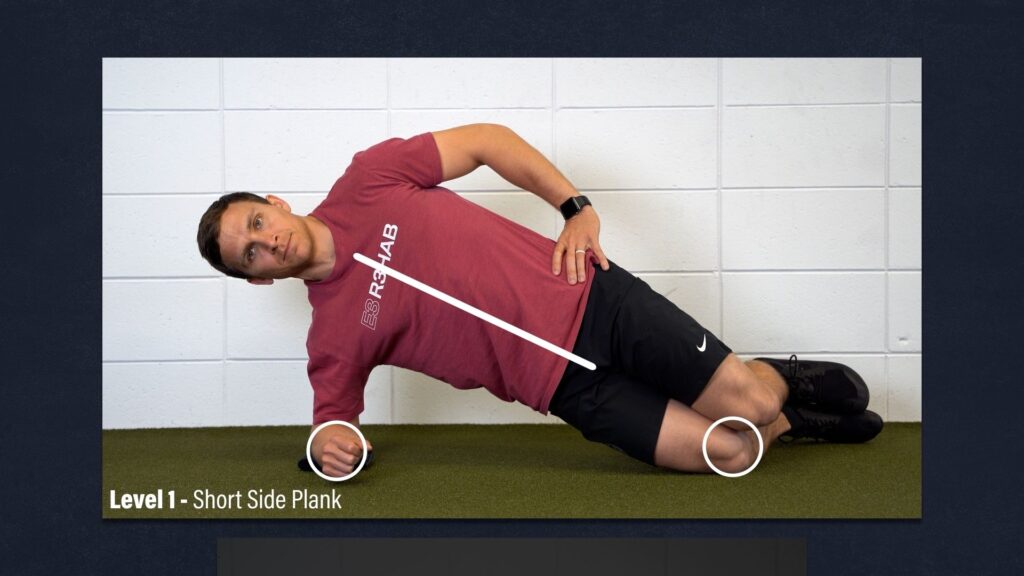
(Anti) Lateral Flexion
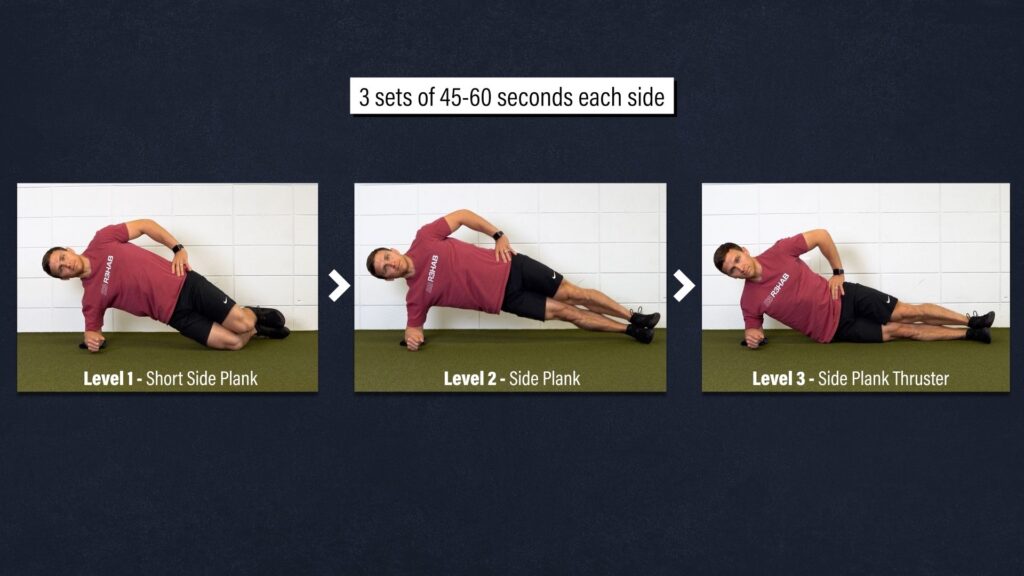
Level 1 – Short Side Plank. Start on your forearm and knees while keeping your trunk in a straight line. Hold this position.
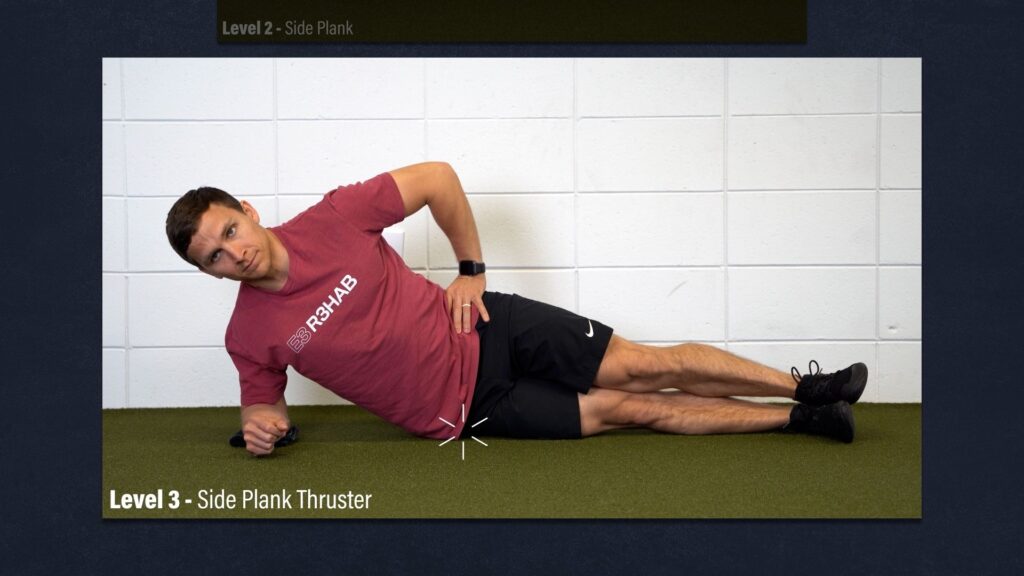
Level 2 – Side Plank. Straighten your legs, stack your feet, and keep yourself in a straight line, both from a front view and top view.

Level 3 – Side Plank Thruster. Position yourself in the same way as the previous exercise, but slowly tap the floor with your hip before returning to the starting position and repeating that motion.
Aim for 3 sets of 45-60 seconds as you work through each exercise.
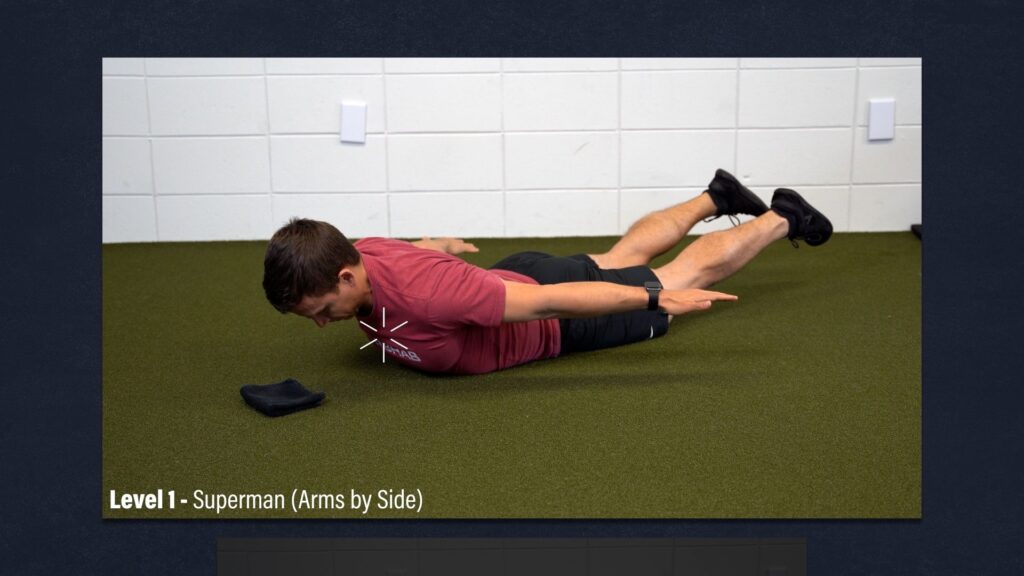
(Anti) Flexion
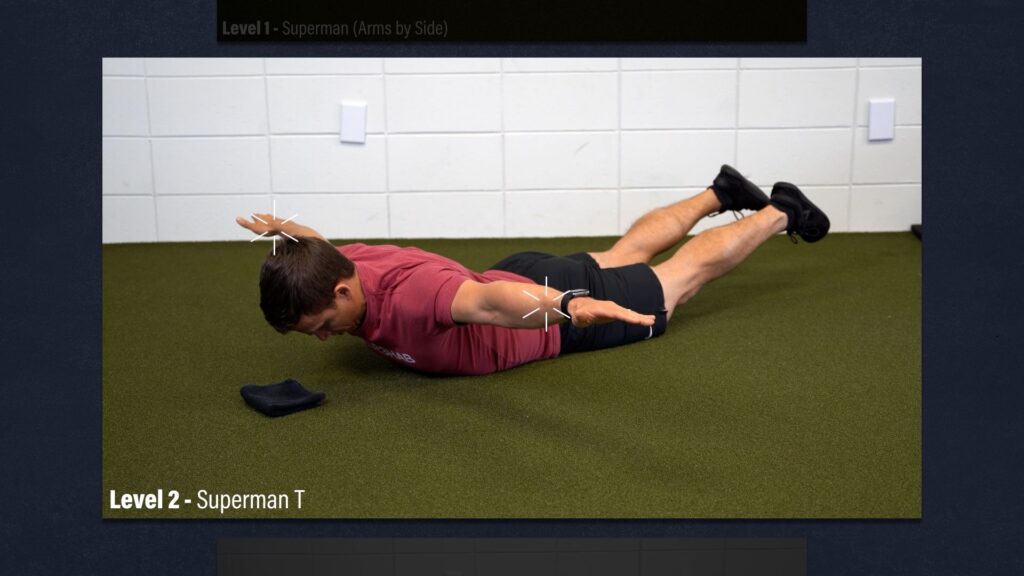
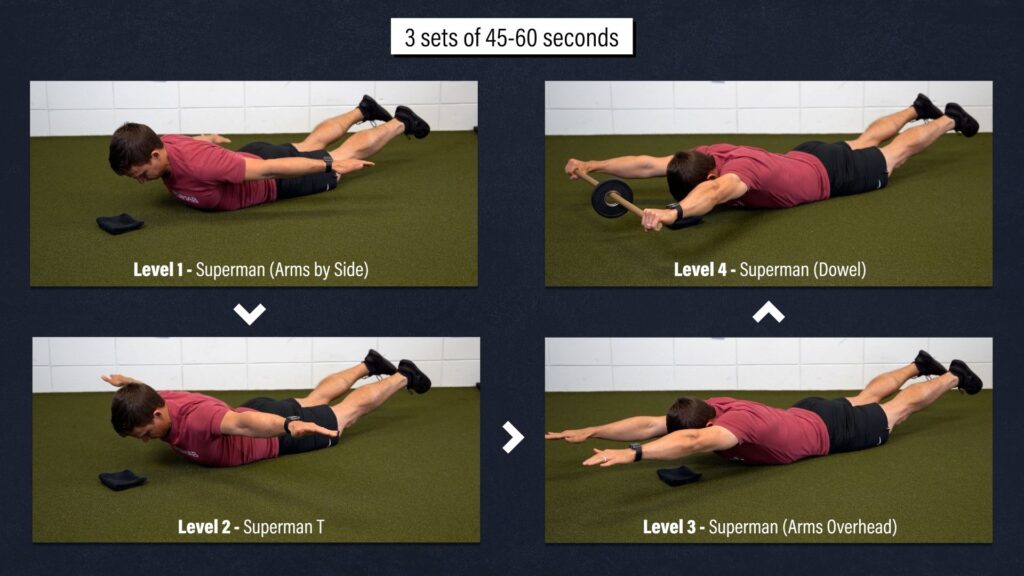
Level 1 – Superman w/ Arms by Side. With your arms down by your side, slowly lift your torso and legs off the floor, only as far as tolerable, and hold this position.
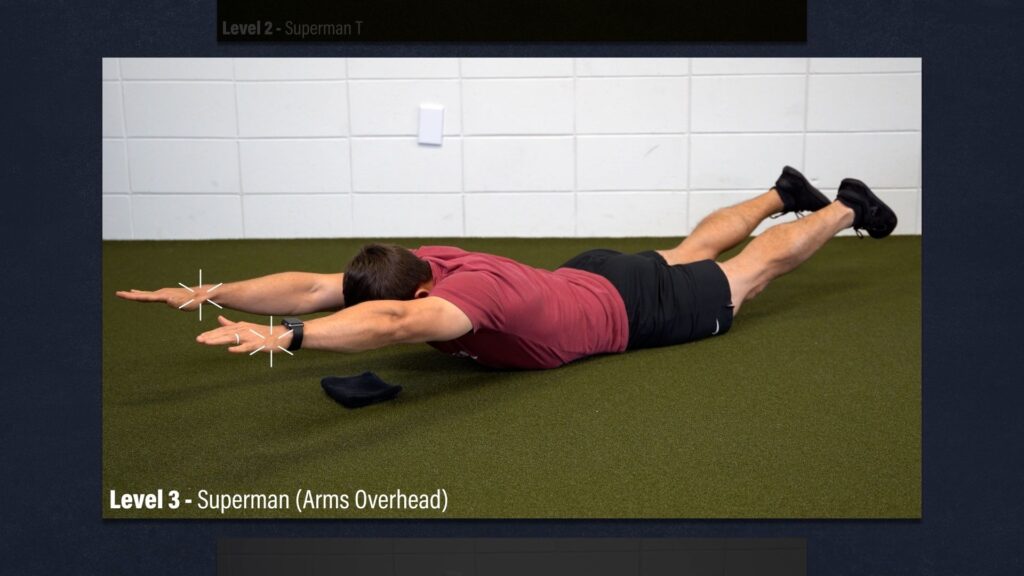
Level 2 – Superman T. The setup and execution will be the same except you’ll have your arms out to the side.
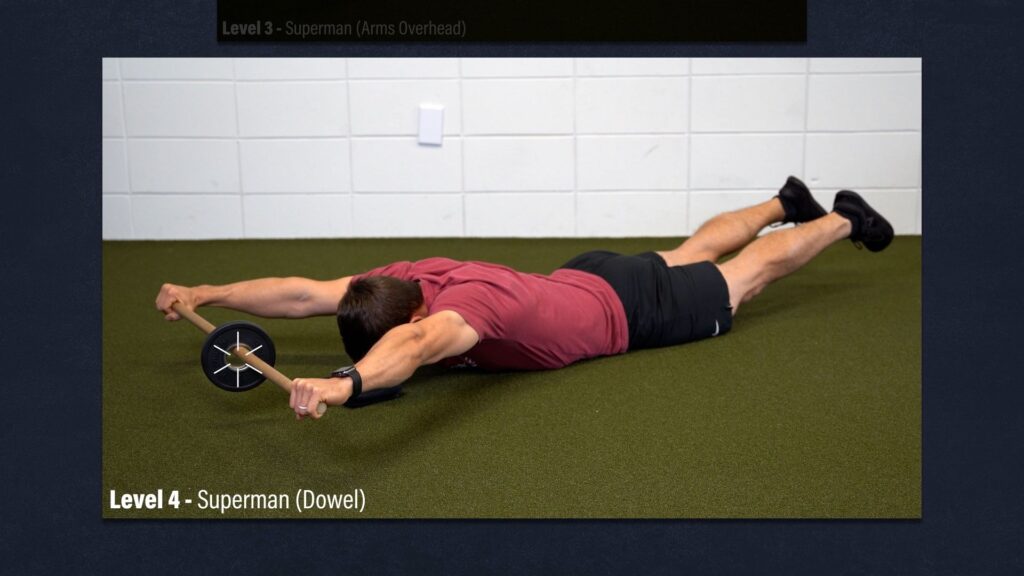
Level 3 – Superman w/ Arms Overhead.
Level 4 – Superman w/ Dowel. Progressively add weight to the exercise to make it more challenging.
Aim for 3 sets of 45-60 seconds as you work through each exercise. Only extend your back as far as comfortable with each movement.
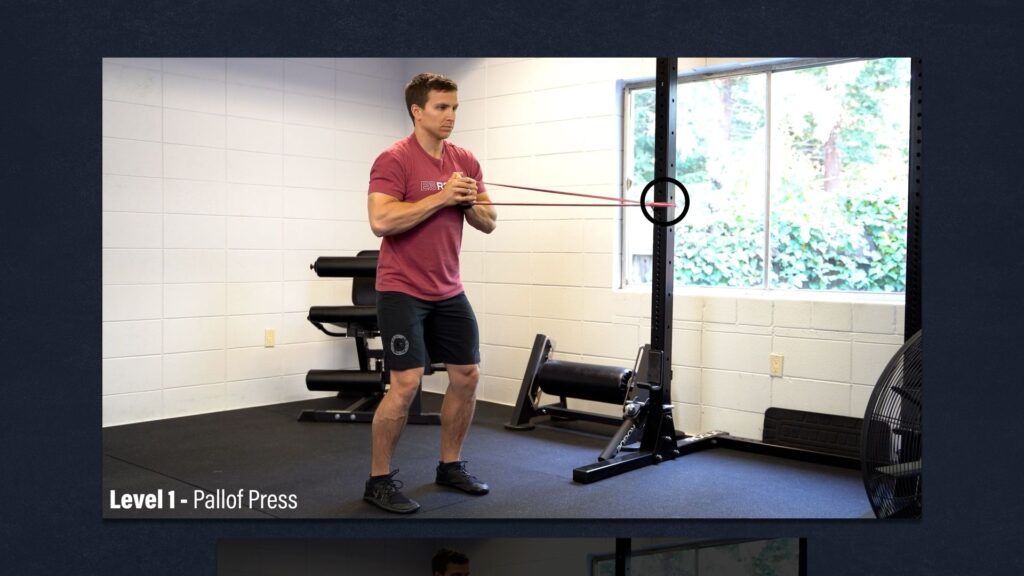
(Anti) Rotation
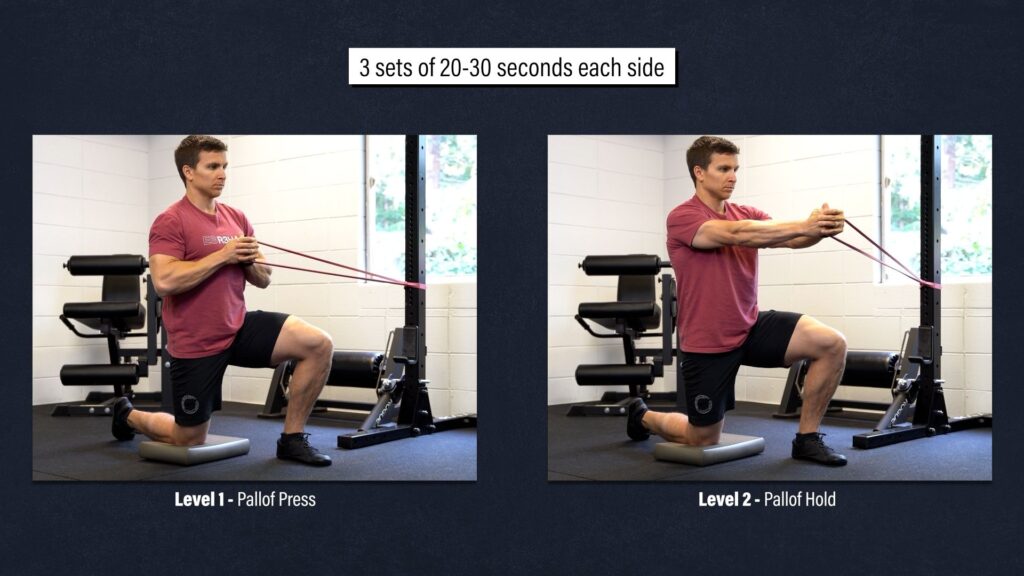
Level 1 – Pallof Press. Start standing with your hips and knees slightly bent, and a band anchored perpendicular to your body at about chest height. Press the band out until your arms are straight, slowly return to the starting position, and repeat.
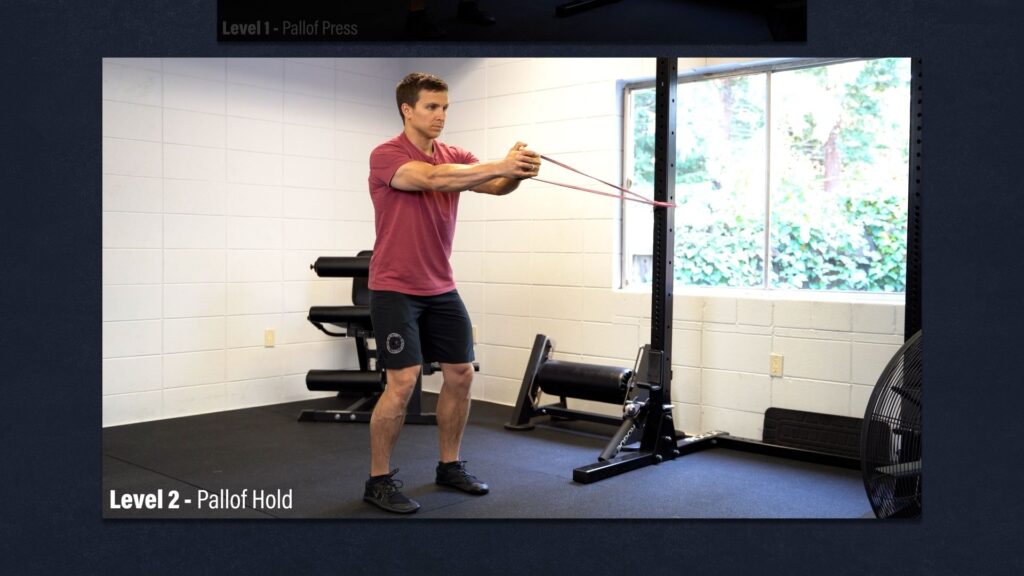
Level 2 – Pallof Hold. Same thing, but hold the band out the entire time. Increase the resistance of the band or step further away to make the exercise more challenging.
Alternatively, and my preference if you can tolerate it, is to do the exercises in a half kneeling position. Aim for 3 sets of 20-30 seconds per side.
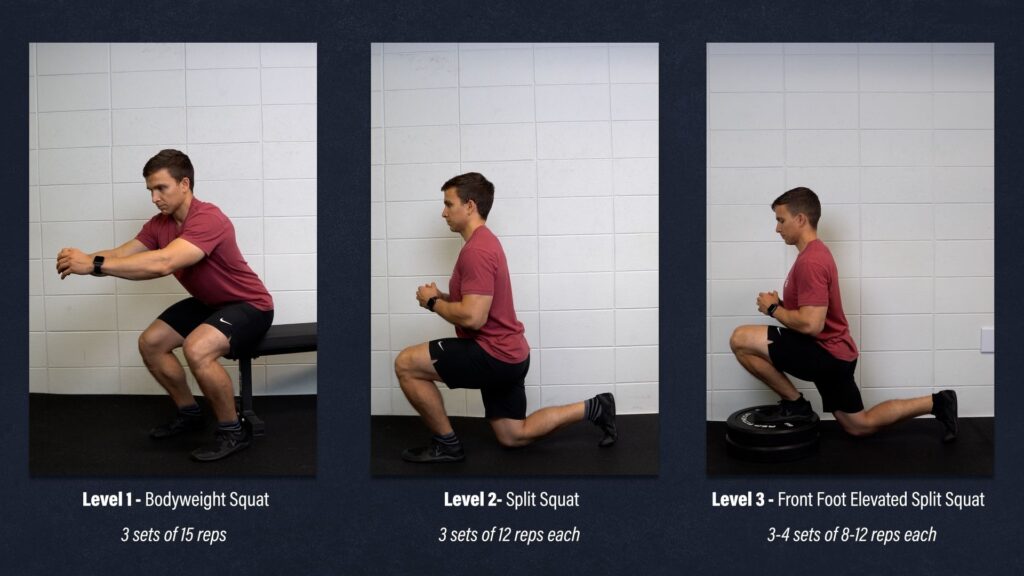
Split Squats
Level 1 – Bodyweight Squat. Gently tap your butt to a chair and stand back up. If it’s too challenging, shorten the range of motion or use your hands for assistance. Aim for 3 sets of 15 repetitions.
Level 2 – Split Squat. Start in a stride stance and lower yourself down so that your back knee taps an egg that you don’t want to crack. If it’s too difficult, shorten the range of motion or use your hands for assistance. Aim for 3 sets of 12 reps.
Level 3 – Front Foot Elevated Split Squat. Elevate the front leg using a 2-4” object. Aim for 3-4 sets of 8-12 slow and controlled reps. Add weight as needed.
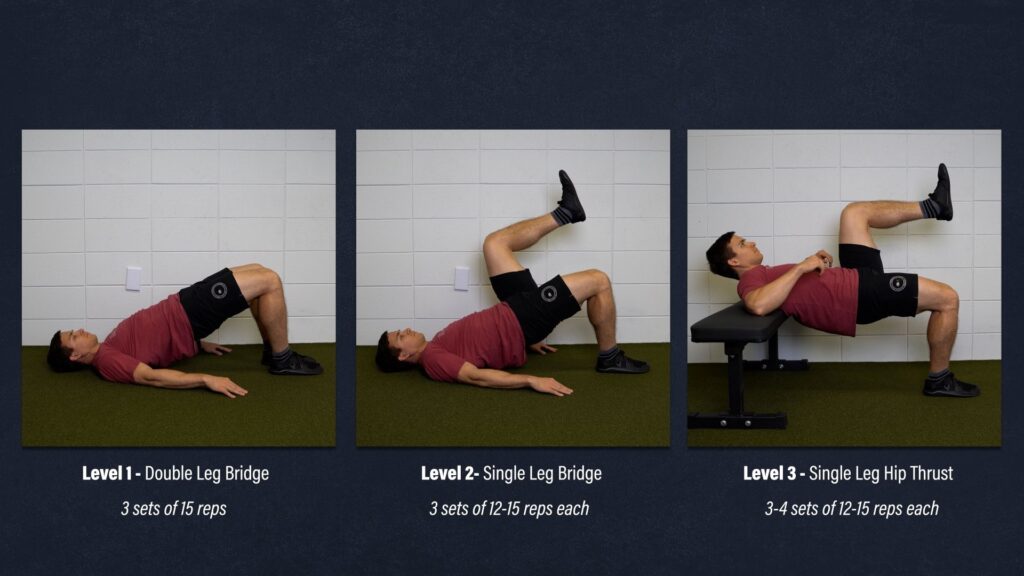
Bridges
Level 1 – Double Leg Bridge. Lie on your back, bridge up, squeeze your glutes, lower yourself down, and repeat. Aim for 3 sets of 15 reps.
Level 2 – Single Leg Bridge. Aim for 3 sets of 12-15 reps.
Level 3 – Single Leg Hip Thrust. Aim for 3-4 sets of 12-15 slow and controlled reps. Add weight as needed.
Guidelines, Not Rules
As always, these exercise recommendations are guidelines, not hard and fast rules. You should get clearance from your medical doctor and tailor the exercise routine to your individual needs.
For example, some individuals may only need to work on a few of the level 1 & 2 exercises presented to accomplish their goals. However, some people might need to include additional exercises like rows, pull-ups, push-ups, presses, deadlifts, etc. based on the activities they’re trying to return to.
Other trunk exercises include medicine ball throws, shoulder taps, suitcase carries, and roman chair or GHD variations.
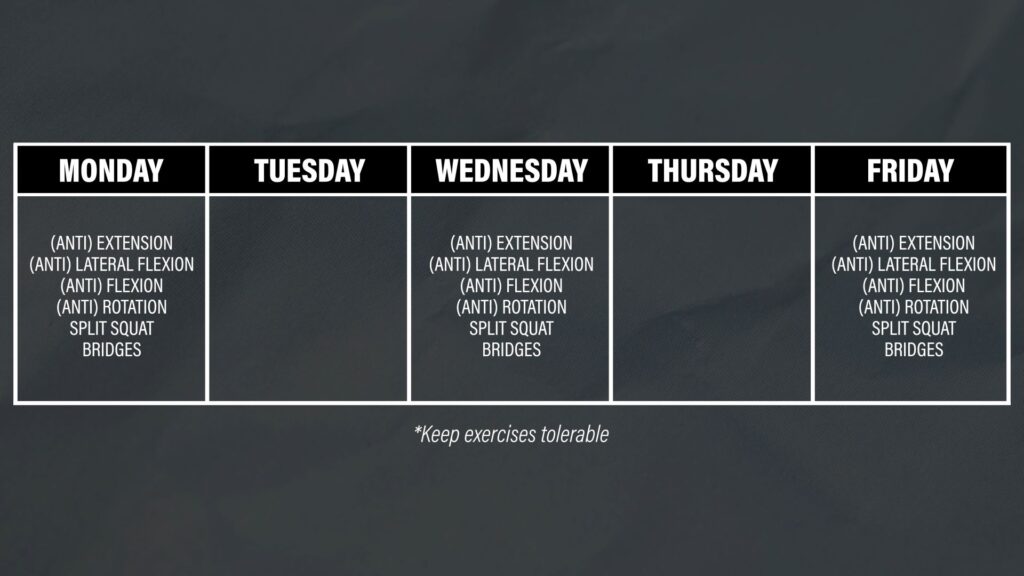
Regardless of what you choose to do, you should aim to train at least 2 to 3 times per week while ensuring that each movement is tolerable.
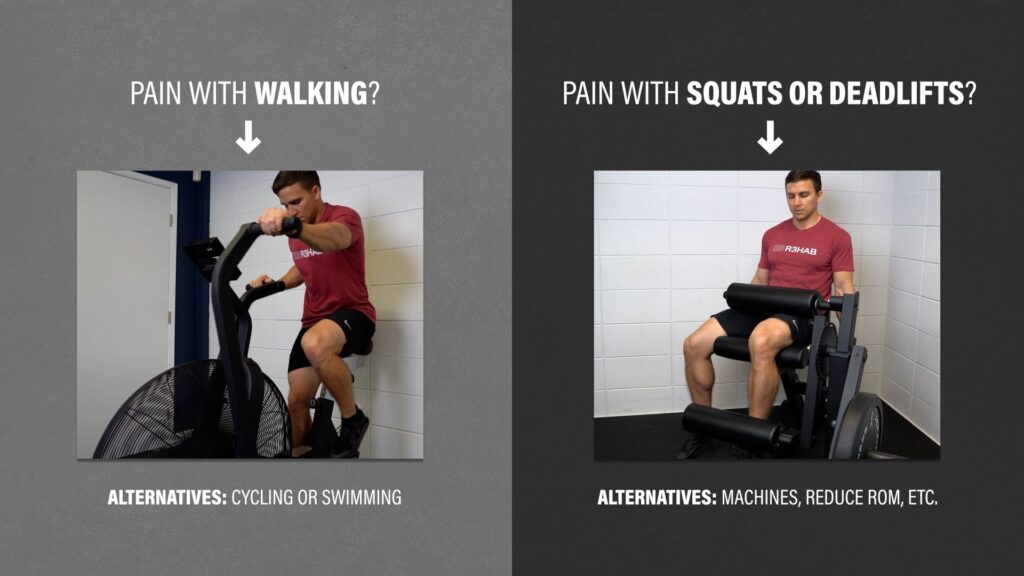
Activity Modifications
In addition to performing the exercises outlined, it’s important to maintain your physical activity levels to the best of your ability.
If walking has become difficult, cycling or swimming can be great alternatives to stay active and minimize deconditioning.
If squats or deadlifts are uncomfortable, you can swap exercises, use more machines, reduce the range of motion, etc.
If your goal is to return to a specific sport, then you need a gradual and progressive plan to get you there. In some cases, such as when a stress fracture occurs due to a repetitive activity, initially taking a break from that sport may be required to allow for healing.
In any case, seek the guidance of a healthcare team.
When Should You Get Surgery?
I can’t give you a definitive answer, but I can provide you with information that you can take into consideration during that discussion with your medical doctor.
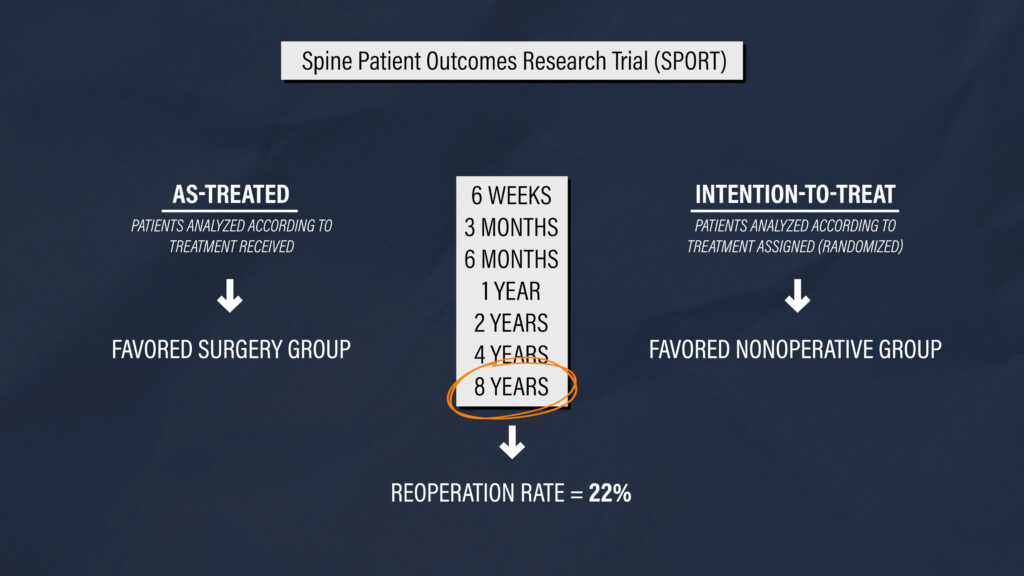
The Spine Patient Outcomes Research Trial (SPORT) compared surgery with nonoperative management for lumbar degenerative spondylolisthesis at 6 weeks, 3 months, 6 months, 1 year, 2 years, 4 years, and 8 years later. The as-treated analysis favored patients managed surgically, while the intention-to-treat analysis favored the group randomized to nonoperative care. The reoperation rate after 8 years was 22%.
A different study by Matsunaga et al in 2000 followed patients managed nonoperatively for 10 to 18 years. There are three big takeaways from this paper:
- Development of neurological deficits was not correlated with progression of slippage.
- The stability of the spine improved on its own for many of the patients.
- The majority of patients who had cauda equina syndrome at the initial examination had a worsening of symptoms.
Therefore, surgery may be indicated in some cases, such as when severe or progressive neurologic deficits are present, but non-operative management is usually the first recommendation.
To date, no randomized, placebo-controlled trials that compare real surgery to fake surgery have been conducted.
Summary
In summary, spondylolisthesis is a condition characterized by displacement of one vertebra relative to another. Since it is present in the asymptomatic population and is poorly associated with low back pain and physical disability, non-operativement management is recommended as the first line of treatment in the majority of cases. Surgery may be indicated if severe or progressive neurologic deficits are present, and this should be discussed with your medical doctor.
Exercises should focus on improving function rather than trying to change the structure of your spine. Examples include trunk and leg strengthening, which can be performed 2 to 3 times per week, or as tolerated. Additionally, modifying or reducing aggravating activities, such as walking, running, deadlifting, and playing various sports is an integral component of the overall rehab process.