

In this article, I’m going to teach you everything you need to know about PCL injuries, including whether surgery is necessary, as well as provide you with a comprehensive rehab program.
Be sure to also check out our Knee Resilience Program!
Anatomy & Function
The posterior cruciate ligament, or PCL, attaches from the femur, or thigh bone, to the tibia, or shin bone and is located just behind the ACL. As the largest and strongest ligament in the knee, it plays a crucial role in maintaining knee stability.
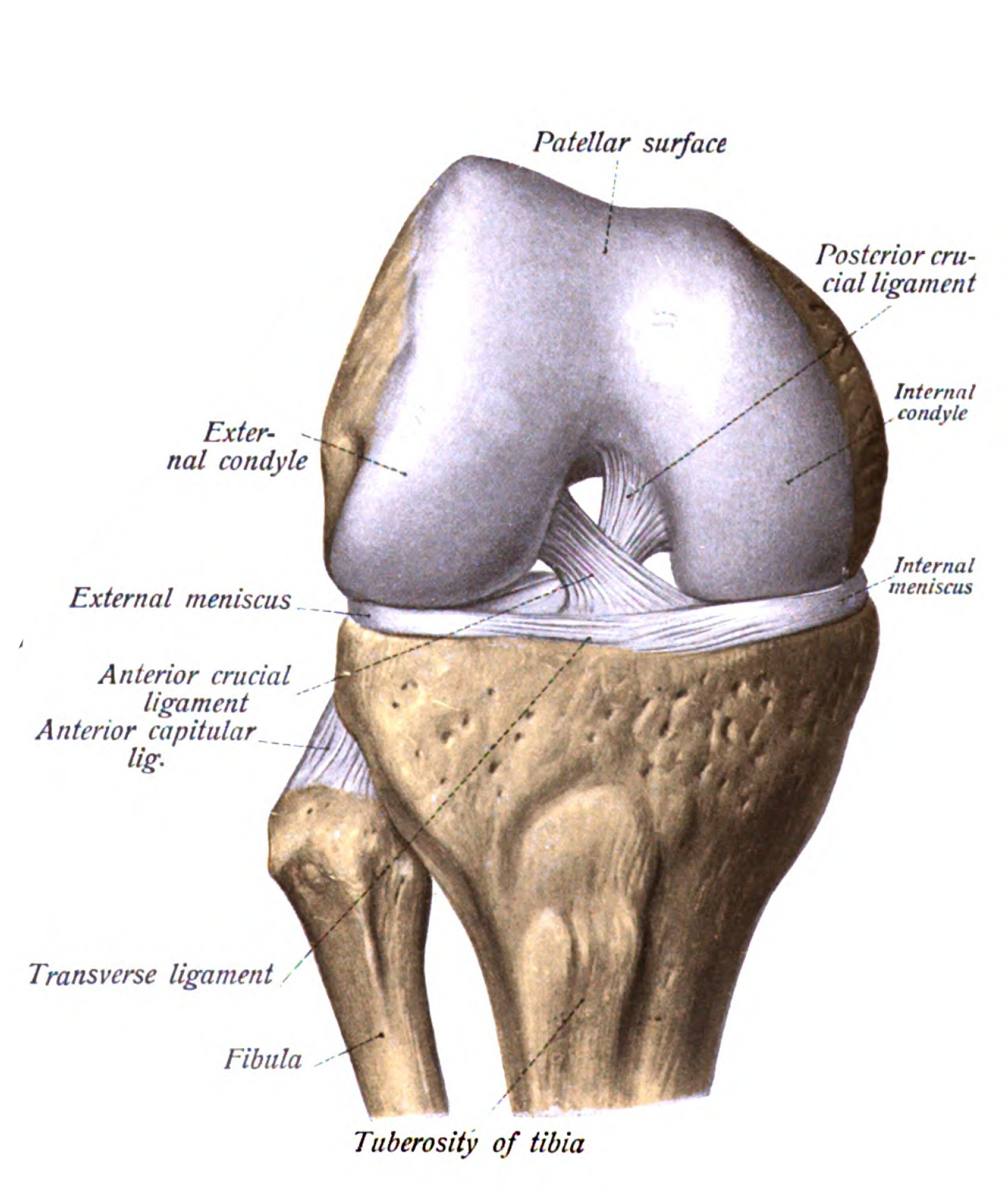
Its primary function is to prevent the tibia from moving backward in relation to the femur, however it also helps stabilize the knee against extreme inward (varus), outward (valgus), and rotational stressors.
PCL Injuries
A PCL injury occurs when a high-energy force causes the tibia to abruptly move backward relative to the femur. The most common causes include motor vehicle accidents when the knee hits the dashboard, or during sports, such as falling onto a bent knee. It can also result from a direct force that causes the knee to hyperextend.
The severity of the injury is typically graded on a scale from 1-3 based on findings from a clinical examination and imaging:
- Grade 1 involves a partial tear of the PCL with minimal joint laxity.
- Grade 2 has a tear greater than 50% and moderate joint laxity.
- Grade 3 has a complete tear of the PCL and significant joint laxity.

Since a PCL injury results from higher forces, they are often associated with other injuries, most commonly involving the ACL, MCL, meniscus, and/or the posterolateral capsule of the knee.
PCL Injury Management
Since the PCL has an intrinsic capability for healing, an isolated tear can be managed nonoperatively with bracing and rehabilitation in many cases. Wang et al 2018, Patel et al 2007, Jacobi et al 2010, Vaquero-Picado et al 2017, Agolley et al 2017
In fact, a 2018 article by Wang et al found that “Nonoperative treatment of isolated PCL injuries results in good subjective outcomes and high rate of return to sport.”
Based on the current evidence, here i s an algorithm for the treatment of PCL injuries:
- For an isolated grade 1 or 2 tear of the PCL, nonoperative treatment is recommended.
- An isolated grade 3 injury can also be treated nonoperatively if symptoms are mild and overall activity demands are low. This means the patient does not intend on participating in sports or activities involving jumping, running, twisting, etc. Wang et al 2018, Kew et al 2022.
- If symptoms and instability continue to persist after conservative treatment for an isolated grade 3 injury, referral to a surgeon would be recommended.
- Finally, if there is involvement of another structure, such as an ACL tear, surgery would be the preferred treatment.

Of course, deciding whether to have surgery is always going to be a bit more nuanced — it depends on factors like the severity of your injury, your function, and your personal goals. It should go without saying, but if you suspect you have a PCL injury, you should consult your surgeon to determine the most appropriate option for your specific situation.
PCL Injury Rehab Overview
Whether or not you have surgery, the goal of rehab is to address the main symptoms and deficits associated with a PCL tear. This involves managing pain and swelling, while improving your knee range of motion, strength, and stability during functional activities. These activities range from daily tasks like going up and down stairs to sport-specific movements such as decelerating, jumping, cutting, and pivoting. Wang et al 2018, Vaquero-Picado et al 2017, Agolley et al 2017
The comprehensive rehab program that I am going to present will consist of 3 overlapping categories of exercises that will focus on improving your knee range of motion, strength, stability, and power.

My intention is that you will use these categories as a framework for programming exercises based on your current function, tolerance, and goals. I’ll provide more details and examples of how you can do this later in this article.
Since isolated PCL injuries typically do not require surgery, the rehab principles in this article are geared toward nonoperative cases. Post-operative rehab will be somewhat similar to nonoperative management, but there are some differences due to factors like healing timelines and post-surgical precautions. For instance, following surgery there are typically weight bearing and range of motion restrictions for a set duration of time to protect the surgical reconstruction. Timelines and precautions may also vary depending on whether other structures were surgically addressed, such as your ACL or meniscus.
Immobilization and Bracing
Before diving into the exercises, I want to quickly discuss 2 main considerations to keep in mind during the initial weeks following a PCL injury.
First, one of your primary goals will be to monitor and manage your knee pain and swelling as best as you can. While icing and elevation can help, the key is actually finding the right dosage of activity and exercise without overdoing it. If you push too hard or too fast too soon, it may cause a flare-up and delay your progress.

This ties directly into the second consideration which is immobilization, bracing, and the use of assistive devices. If you’re unable to fully bear weight while walking, crutches may be used initially to manage your pain and swelling by offloading the knee joint.
Additionally, you will likely wear a knee brace since it is recommended for nonoperative cases and is required following surgery. The most common type is called a dynamic PCL brace. This has a spring mechanism that applies a constant, forward force on the tibia, placing the PCL in a more optimal position for healing. Your doctor may also recommend that the brace is locked into extension for a set duration of time. There are generally 2 main reasons for doing this:
1. It prevents you from bending the knee too much too early, since deeper knee flexion may place more strain on the PCL.


Therefore, locking the brace into knee extension theoretically gives the PCL a better chance to heal.
There’s no set guideline on how long to keep the knee brace locked or how long to wear the brace. However, based on a handful of studies looking at nonoperative management, most authors recommend about 2-4 weeks in full extension, and wearing the brace for anywhere between 12-16 weeks following the injury.
If you had surgery, this timeframe is highly variable depending on your surgeon’s protocol and if other structures were involved, but some recommendations will have the brace locked in extension for about 3-6 weeks and continuing using the brace for up to 4-6 months or longer.
Category #1: Range of Motion Exercises
This involves restoring your knee extension and flexion range of motion.

For knee extension, your goal is to get your knee completely straight, or close to it, as soon as possible. Depending on your previous range of motion, you may even achieve a few degrees of hyperextension.


However, for more severe injuries and following surgery, it’s recommended to avoid pushing into hyperextension early on since this can place more strain on the PCL.
To improve your knee extension, the main exercise you will want to perform early and often is quad sets. Whether you are sitting or lying on the floor, straighten your leg as best as you can and then squeeze your quadriceps, the muscles on the front of your thigh. Hold for 10 seconds, relax, and repeat 10 times.

When it’s appropriate to do so, more advanced variations include using a strap to pull up on your foot and propping your heel on a small object in order to move through more range of motion. You can perform these quad sets multiple times a day, every day.

For knee flexion, normal range of motion is generally around 135°, or being able to bring your heel to your butt or very close to it. If you had surgery, you will likely have restrictions against how much knee flexion you are allowed in the first few weeks, so it’s important you follow your surgeon’s recommendations.

Also, as I mentioned earlier, one of the early goals of rehab is to minimize hamstring activation through larger ranges of knee flexion. Therefore, here are two exercises to help restore knee flexion with minimal hamstring contribution.
Option 1: Scooting Knee Flexion. Sit in a chair with your foot flat on the ground, then use your arms to scoot your hips forward, which will help bend your knee further. Perform for 2-3 sets of 30-60 second holds.

Option 2: Seated Heel Slides. Sit on the edge of a chair and place your foot on a slider if you’re on carpet or a towel if you’re on a hard surface. Using your other leg, gently slide your foot backward, trying to bend your knee as much as you can. Hold the end position for a few seconds, then return to the starting position. Repeat for 2-3 sets of 10-20 repetitions.

Once symptoms and function allow, or as your surgeon reduces restrictions, you can progress to assisted heel slides and riding a stationary bike.
For the heel slides, lie on your back, wrap a towel or strap around your foot, and gently pull on it, sliding your heel toward your butt. Perform this exercise for 2-3 sets of 10-20 repetitions.

And finally, the last option is riding an upright stationary bike. Depending on your knee range of motion, you might start by performing half revolutions with the seat high. You can progress by lowering the seat and completing full revolutions. You can do this for anywhere between 5-30 minutes, daily, as tolerated.

Category #2: Strengthening Exercises
The main focus will be on restoring your quadriceps and hamstrings strength. However, if you are looking for a more comprehensive program, I’m also going to review three additional groups of exercises: one focused on strengthening your calves, another targeting your hips and trunk, and a third aimed at improving dynamic balance.

The first group involves strengthening your quadriceps since they are important for improving your knee function and stability, as well as reducing the risk of future injuries.
In addition to the quad sets mentioned earlier, you’ll also perform straight leg raises in the early stage of rehab. Lie on your back with one knee bent, straighten the other by squeezing your quads, and lift until your thighs are in line with one another. Slowly control back down. An important milestone is being able to perform this movement with your knee completely straight. Once you can do that, build up to 3 sets of 10-20 repetitions.

Other options for strengthening the quadriceps include squats, step downs, and gym based exercises like a leg press.

Many protocols recommend performing these exercises with a limited range of motion early on, as deeper knee flexion can put more strain on the PCL. However, there is no universal consensus for how deep you should go or for how long these restrictions should last. Your physical therapist might progress these movements based on your function and tolerance, while in surgical cases, you will have restrictions based on your surgeon’s protocol.
Regardless, these exercises will generally start with less range of motion and intensity, and gradually progress over time. For example, the leg press can be performed with two legs through a partial range of motion – which avoids deeper knee flexion – and can be progressed by performing with a single leg, and eventually moving through your full range of motion.

For squats, here is a simple progression I like to use. While holding onto a stable object for support, gently tap your butt to a pad or pillow placed on top of a chair or box, then stand back up. To make this more challenging, you can perform these without upper body assistance. Eventually, you will remove the pad or pillow so you move through more range of motion. And if you want to make them harder, you can hold a weight in your hands.

When cleared to do so, you can remove the chair or box and perform bodyweight squats to a comfortable depth.

These can be progressed by adding weight in the form of a dumbbell, kettlebell, barbell, etc.

Ultimately, you can sit into an even deeper, more upright squat by elevating your heels. One of the chief complaints after a PCL injury is pain in the back of the knee when sitting in a deep squat, so carefully improving your tolerance to this position over the course of your recovery can be helpful.

In addition to squats, you will include single-leg exercises to address asymmetries in strength while improving stability and control on each leg. Here are 2 progressions:
Option 1: Split Squats. Start in a stride stance and slowly lower yourself down to a pad or object, before standing back up. If you need to make these easier, use your hands for assistance. Over time, you can make them more challenging by removing the pad, and then eventually holding a weight in your hand.

If you are looking for a more advanced variation, you can try elevating your front foot so you move through more knee flexion range of motion.
Since a main deficit after a PCL injury is difficulty and apprehension with deceleration, incorporating forward lunges can be beneficial for athletes looking to return to field and court sports.
Just like the front foot elevated split squat, this will place increased strain on the PCL and therefore should be reserved for the later stages of rehab.

Another common issue following this injury is difficulty with descending stairs and walking downhill. That leads me to the second single leg progression: step downs. Start with step ups at a lower height either with or without your hands for assistance. Over time, you can gradually increase the height of the step. From here, you can stand sideways and perform lateral step downs or face forward and perform forward step downs. To make these harder, increase the height of the step.

Another option for quad strengthening is leg extensions. Your physical therapist might have you start with two legs through a partial range of motion in order to avoid deeper knee flexion angles.

Over time, progressions include using a single leg and moving through your full range of motion.

If you don’t have access to a leg extension machine, you can do isometrics with a band for 3-4 sets of 15-45 second holds, provided you’re cleared to perform exercises with more knee flexion.

All of these quadriceps exercises can be performed anywhere from 3-4 sets of 5-20 repetitions, depending on the stage of rehab and desired adaptation. For the single leg exercises, you will perform them on both legs.
The next group of exercises will focus on strengthening your hamstrings.
As I mentioned earlier, there is research showing that contracting the hamstrings at knee flexion angles greater than 10-30° increases strain on the PCL. This means that theoretically a prone hamstring curl through your full range of motion will be more strenuous on the PCL than an isometric prone hamstring curl performed with the knees in a more extended position.

This is the main reason why so many protocols restrict knee flexion-based hamstring strengthening in the early stages of rehab. For example, this literature review of various surgical protocols found that the recommended initiation of resisted hamstring exercises varied from 6 weeks to up to 4 months or longer following PCL surgery.

Again, your physical therapist might start and progress hamstring exercises based on your function and tolerance. If you had surgery, you will eventually perform the same exercises but you will have restrictions based on your surgeon’s protocol that may limit hamstring strengthening for up to 3-4 months. This is important because this means you will have to work very hard on regaining your hamstring strength in the later stages of rehab, especially if you want to return to sport.
A general starting point will be performing isometrics with the knee in a more extended position since this places little to no load through the PCL. For instance, you can lie on your back, straighten your legs so your knees are slightly bent, then dig your heels into the ground and think about pulling them toward your butt.

If you have access to a prone hamstring curl machine, you can load up the weight stack and perform an isometric by driving your ankles into the pad at a tolerable effort level. You can do this with two legs or a single leg.

When symptoms and function allow, or you are cleared to do so, you can perform knee flexion strengthening through your full range of motion. This can be done using the prone hamstring curl machine, a seated hamstring curl machine, or on an exercise ball.

Start with a double leg variation and progress to a single leg over time.

Another option is this slider progression. Start with double leg eccentric only, progress to double leg through your full range of motion, then single leg eccentric only, and finally on a single leg through your full range of motion.

Some athletes may even want to include advanced options like the Nordic hamstring curl in the later stages of their rehab.

Since the hamstrings also contribute to hip extension, you can incorporate movements in which the knees remain relatively straight. These should place less strain on the PCL, so they can be initiated as your symptoms and function allow.
Options include Romanian deadlifts and roman chair hip extensions either with two legs or with a single leg.

You can also work your way through a feet elevated long lever bridge progression. Start with two legs, progress to an eccentric variation where you bridge up on both legs, remove one leg then slowly lower down, and finally you can perform on a single leg.

Similar to quadriceps strengthening, these hamstring exercises can be performed for 3-4 sets of 5-20 repetitions or 15-45 second holds for the isometrics. Again, if you are doing a single leg variation, you will perform the exercise on both sides.

For those looking for a more comprehensive program, here are 3 additional groups of exercises you can include in your rehab program.
For the calves, a simple standing progression starts with two legs on flat ground and progresses to a single leg on a step with weight.

You can also perform seated heel raises using a machine or with weights on your knees either with your feet on the floor or on a step.

For the hips and trunk, there are endless options but some examples include double leg and single bridges and hip thrusts, short side planks, regular side planks, and side lying hip abduction with or without resistance.

And lastly, you might want to consider adding dynamic balance exercises to help improve your tolerance to rotational and lateral stresses.
Once you can stand on a single leg for at least 30 seconds without losing balance, here are 3 options you can progress to.

Option 1: 3-Way RDL. Start with a single leg RDL without letting the other foot touch the ground. From here, progress to a 3-way RDL, where you reach your arms in 3 directions – to the left, middle, and then to the right. And finally, you will progress the previous movement by adding a knee drive.

Option 2: Y Balance. Stand on one leg and then reach your opposite foot in three different directions, creating a Y shape. You can start with smaller distances, but if you want to make it more challenging, try reaching as far as you can in each direction.

Option 3: Single Leg Rotation. Stand on one leg, rotate your torso as far as you can in one direction, and then rotate as far as you can in the other direction. Start with small rotations and work up to your full range of motion. To make this more challenging, you can add resistance by holding a band.

Any of these dynamic balance options can be performed for 3-4 sets of 30-60 seconds on each leg.

Category #3: Plyometric Exercises
There is limited data on what criteria must be met prior to initiating plyometric exercises following a PCL injury. However, based on a few surgical protocols, some recommendations include possessing full, pain-free knee range of motion, the ability to demonstrate a good quality single leg step down, and quadriceps and hamstring strength of at least 75% compared to the uninjured side. These are actually similar recommendations for beginning plyometrics after an ACL reconstruction.

There are endless options to choose from, but I am going to show you 2 progressions and explain the rationale for each.
The first option is a vertical jump progression since they have been shown to be better suited for improving overall knee function.
Level 1: Box Jump. Start with a box jump since this will reduce landing impact forces.
Level 2: Vertical Jump. Perform a vertical jump, building up to a maximal effort.
Level 3: Depth Drop. Step off an elevated surface and land on two legs.
Level 4: Depth Jump. Step off, land on two legs, and then quickly jump up as high as possible.
Level 5: Single Leg Depth Drop. Step off an elevated surface and land on one leg.
Level 6: Single Leg Depth Jump. Land on one leg, then immediately jump up as high as you can.

In this progression, you can make any level easier by reducing the height of the box and/or reducing the effort of each jump. However, your goal is to use an elevated surface about 12 inches high and/or jump at maximum effort before progressing to the next level.


The second option focuses on deceleration since this is a common difficulty seen in athletes following a PCL injury.
Level 1: Forward Lunge. Just like the exercise presented earlier, perform a slow and controlled lunge with an emphasis on driving the knee forward.
Level 2: Forward Lunge with Step Back. Same as previous, but after controlling the deceleration, you will push back to the start with power.
Level 3: Forward Step & Land. Jump forward off one leg and land on the other with control. Step back and repeat.
Level 4: Forward Step & Land with a Jump Back. Jump forward, land on the other leg, then quickly jump back to the start.
Level 5: Running with a Step Back.

Obviously these are only some examples. If you want to learn about other plyometric exercises, you can read this article.
To program these in the simplest way possible, you can aim for 2-4 sets of 4-10 repetitions, 2-3 days per week. However, understand that programming will ultimately need to be customized based on your function, symptoms, tolerance, goals, etc.

Individualizing Your Program
If you have made it this far, you might be wondering how you can put all of this information together. Let me provide 4 additional considerations and examples.
1. These exercises are only some options as the possibilities for exercise selection are limitless.
2. Timelines and rate of progression vary from person to person. This is influenced by your symptoms, tolerance, and function. However, if you had surgery, you will also have to wait until restrictions are lifted by your surgeon or physical therapist.
3. As I said at the beginning – these categories will have overlap. For instance, even once you begin the plyometrics, you will still be performing the quadriceps and hamstring strengthening exercises.

4. You don’t have to do every exercise or exercise category. To demonstrate what I mean, let me show you 2 sample programs for different patients in the later stages of rehab.
The first patient injured their PCL in a car accident and only wants to be able to return to daily activities. Therefore, they might only focus on restoring their knee range of motion and including functional strength exercises like squats and step downs, 2-3 days a week.

On the other hand, a younger athlete looking to return to sport may incorporate all of the exercise categories presented. This includes progressing to the advanced strength movements like forward lunges and Nordic Hamstring curls, other exercises targeting the calves, hips, and trunk, the dynamic balance options, and the plyometric progressions. Since they are doing more volume overall, they may decide to split these exercises across 2-4 days a week.

This athlete will also need to understand how to safely return to running and sport.
Return to Running & Sport
Running can be initiated when you meet the criteria for starting plyometrics.

This usually starts with walk-to-jog intervals on a treadmill and progresses to continuous jogging before slowly ramping up to faster running speeds.

This straight-line running on a treadmill will eventually turn into full sprints, cutting, and multi-directional drills. These are crucial for exposing your knee to lateral and rotational forces at progressively faster speeds.
Returning back to sport will also follow a gradual progression. An article by Kew et al. in 2022 looked at return to play after PCL injuries and noted 4 common criteria:
1. Demonstrates quadriceps strength >90% of the uninjured leg.
2. Has no evidence of instability or giving way.
3. The athlete is psychologically ready.
4. Demonstrates >90% function on return to sport testing.

Based on the precautions with knee flexion-based hamstring strengthening, I also think an athlete should be able to demonstrate hamstring strength >90% of the uninjured leg to help maximize return to sport and reduce the risk of future injuries.

Understand that when you return to sport, this doesn’t mean you are immediately returning to full competition. Since data on PCL injuries is currently lacking, I like this progression from Brinlee and colleagues when returning athletes back to competition following an ACL reconstruction:
- It begins with non-contact practice, followed by small-sided contact practices, then full practice, return to competition with a restricted workload, and finally, return to competition without restrictions.
- An athlete should be able to work through these steps without apprehension, pain, instability, effusion, or compensations.

The takeaway here is that you are gradually increasing the intensity, volume, and complexity of your training. If you haven’t played your sport in months to years, that’s a lot of work that you need to make up.
Do you want a structured plan that’s going to provide you with the knowledge and tools to feel more confident, capable, and resilient than ever before? Check out our Knee Resilience Program!

Thanks for reading. Check out the video and please leave any questions or comments below.
Want to learn more? Check out some of our other similar blogs:


