The purpose of this blog is to answer several questions – 1. What is the scapulohumeral rhythm? 2. What is scapular dyskinesis? 3. Does scapular dyskinesis matter? 4. Does scapular dyskinesis predict injury? 5. Do we need to change scapular kinematics during rehabilitation? 6. What are some practical recommendations?
Looking to improve the strength, range of motion, and control of your shoulders to enhance your function and performance? Check out our Shoulder Resilience program!
Shoulder Anatomy
The shoulder consists of four relevant joints:
- Glenohumeral: The glenohumeral joint (GHJ) is the ball and socket joint that most individuals associate with the shoulder. It is the articulation between the head of the humerus and glenoid fossa/cavity of the scapula (shoulder blade). Primary motions include flexion and extension, abduction and adduction, internal and external rotation, and horizontal abduction and adduction.
- Scapulothoracic: The scapulothoracic joint is not a true joint, but it is used to describe the relationship between the scapula and the thorax. Primary motions include upward and downward rotation, elevation and depression, and protraction and retraction. The scapulothoracic “joint” actually takes its motion from the combination of the two following joints:
- Acromioclavicular: The acromioclavicular (AC) joint is the connection between the lateral projection of the clavicle (collarbone) and the acromion of the scapula. Primary motions include upward and downward rotation, internal and external rotation, and anterior and posterior tilting.
- Sternoclavicular: The sternoclavicular (SC) joint is the articulation between the medial portion of the clavicle and the sternum. Primary motions include elevation and depression, protraction and retraction, and anterior and posterior rotation.
Now that you’ve had a brief review of the relevant shoulder anatomy and the primary motions exhibited, a short history of the scapulohumeral rhythm will be discussed.
Scapulohumeral Rhythm
The scapulohumeral rhythm was first described by Codman in 1934, but it was widely popularized as a term by Inman and colleagues in 1944. The scapulohumeral rhythm refers to the four joints working together to produce motion at the shoulder. Using roentgenography (x-ray image) and the insertion of bone pins into a single subject, Inman determined that the normal scapulohumeral rhythm consists of a 2:1 ratio of movement between the glenohumeral and scapulothoracic joints. For example, to achieve 180 degrees of abduction, 120 degrees would come from the glenohumeral joint and 60 degrees from the scapulothoracic joint. This is simplified a bit for the purpose of this blog, but that’s the general idea and what is commonly taught at universities.
Overall, there are several motions that must take place in order for someone to achieve full shoulder abduction:
- Glenohumeral joint: Abduction (primary) and external rotation (secondary)
- Scapulothoracic Joint: Upward rotation (primary)
- Acromioclavicular Joint: Upward rotation, posterior tilting, and external rotation* (there is variation in the amount of internal/external rotation)
- Sternoclavicular Joint: Elevation, retraction, and posterior rotation
While this information is all well and good, there are substantial disparities in the literature. Let’s go down a rabbit hole and examine various considerations as it relates to the “normal” scapulohumeral rhythm:
- Plane of Motion: Scapulohumeral rhythm can differ based on the plane of motion. For example, Ludewig et al. 2009 stated that “the average overall scapulohumeral rhythm was 2.1:1 for abduction, 2.4:1 for flexion, and 2.2:1 for scapular plane abduction.” There is also often differences in these numbers between papers.
- Loaded vs Unloaded: McQuade and Smidt 1998 demonstrated that scapulohumeral rhythm varies between loaded and unloaded conditions within asymptomatic males.
- Age: Habechian et al. 2014 and Dayanidhi et al. 2005 both reported that scapular kinematics and the scapulohumeral rhythm differ between asymptomatic adults and children.
- Fatigue: Madsen et al. 2011, Rich et al. 2016, Zago et al. 2020, and Andres et al. 2020 have all demonstrated changes in scapular kinematics following a fatiguing protocol, including in competitive overhead athletes who are asymptomatic.
- Athlete vs Non-Athlete: Hosseinimehr et al. 2015 reported differences in scapulohumeral rhythm between healthy professional overhead athletes (handball and volleyball) and non-athletes.
- Type of Athlete: Struyf et al. 2014 demonstrated that differences exist between overhead athletes who play different sports.
- Gender: Habechian et al. 2016 reported a difference in scapular kinematics between asymptomatic adult males and females.
- Dominant vs Non Dominant Hand: Mastuki et al. 2011 and Schwartz et al. 2014 have shown asymmetries in scapular motion between dominant and non-dominant shoulders within individuals.
- Non-Linear: Many papers show the non-linear relationship of the scapulohumeral rhythm throughout the range of motion. For example, McQuade and Smidt 1998 demonstrated that the scapulohumeral rhythm can range from 7.9:1 to 2.9:1. The ratio at 60 degrees might be different than 90 degrees which might be different than 120 degrees which might be different than 150 degrees. It’s not a perfect ratio throughout the entire arc of motion.
- Injury and Pain: Individuals diagnosed with shoulder impingement or rotator cuff pathology, glenohumeral joint instability, and adhesive capsulitis can have alterations in scapular kinematics during arm elevation compared to healthy controls. However, the changes are not always predictable. For example, they may have increased, decreased, or no change in scapular upward rotation as reported by Ludewig et al. 2009. Which came first: the chicken or the egg? We’ll touch on this more later.
- Other Factors: There is a lot of heterogeneity in how shoulder motion is assessed between papers. Patient position: seated vs standing? Speed: 2-3 seconds up and down or patient preference? Plane of motion/angle? Weighted vs unweighted? The list is long.
As you can see, there are a lot of individual factors that might influence an individual’s scapulohumeral rhythm. Imagine how all of these things interact.
Scapular Dyskinesis
While the type of motion at each joint is fairly predictable with reaching overhead, the previous section hopefully highlights why the exact scapular kinematics and corresponding scapulohumeral rhythm might be slightly more unpredictable. Scapular dyskinesis is a phrase that translates to “abnormal motion” of the shoulder blade. However, if we have a difficult time defining “normal,” how do we define “abnormal?”
Kibler et al. 2002 created a scapular dyskinesis system to categorize scapular motion into 4 types (arm elevation was assessed from a posterior view):
Type 1 (Inferior Angle): “Type I dyskinesis is prominence of the inferior medial scapular angle, representing loss of scapular control about a horizontal axis parallel to the scapular spine.” Clinically, this is often attributed to tightness of the pectoralis minor and/or weakness of the lower trapezius (more on this later).
Type 2 (Medial Border): “Type II is prominence of the entire medial scapular border, representing loss of scapular control about a vertical axis parallel to the spine.” Clinically, this is often attributed to weakness of the serratus anterior.
Type 3 (Superior Border): “Type III is prominence of the superior scapular border, representing excessive upward movement of the scapula and loss of control around a sagittal axis through the scapula.” Clinically, this is often attributed to over-activation of the upper trapezius.
Type 4 (Symmetric Scapulohumeral Motion): “Type IV is considered to be symmetric scapulohumeral motion, with no prominence or excessive motion relative to the uninvolved shoulder.” This is deemed normal motion.
Uhl et al. 2009 attempted to refine this system to a simple yes/no method to increase the inter-rater agreement, sensitivity, and positive predictive value, as well as allow for assessment of multi-planar motion compared to the original 4-type method – “yes” was given for any dyskinesis noted or “no” for no abnormal motion present.
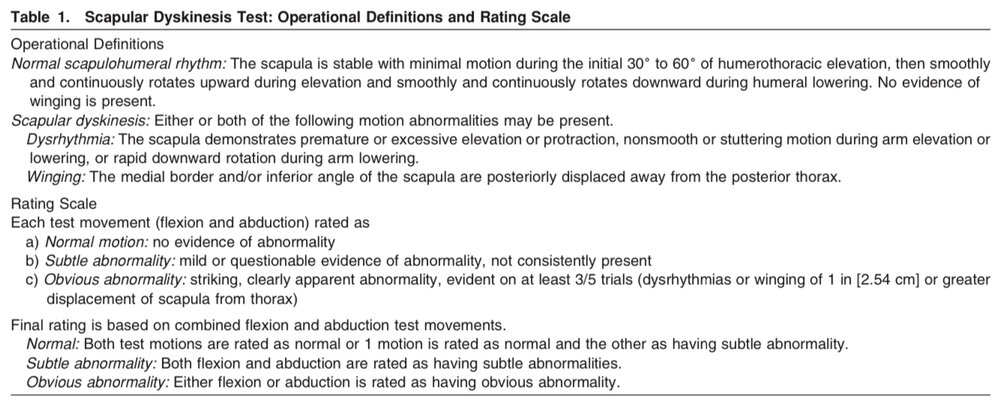
Simultaneously, McClure et al. 2009 and Tate et al. 2009 were developing their own scapular dyskinesis test (SDT) in which participants performed 5 repetitions of bilateral, active, weighted (3 and 5lbs depending on the weight of the subject) shoulder flexion and abduction using a “thumbs up” position (raising up to the count of 3 and lowering to the count of 3). As you can see below, the operational definitions used by these authors differed from that of Kibler and Uhl. Normal motion, subtle abnormality, and obvious abnormality were used to categorize scapular motion (as opposed to the yes/no or the 4 type system) based on the observation of scapular dyskinesis (further broken down into dysrhythmia or winging).
Even if these assessments were flawless (they are not), are we actually identifying “abnormal” motion? Can we predict injury? Can we change the motion? Do we need to change the motion? Read on.
Chicken, Egg, Beneficial Adaptation, or Does it Even Matter?
Which came first: the chicken or the egg? Or, in our case: pain or scapular dyskinesis? Does scapular dyskinesis cause pain/injury or does pain/injury cause scapular dyskinesis? Both? Neither? Does the way you walk cause you to develop plantar heel pain or does plantar heel pain (commonly referred to as plantar fasciitis) cause you to change the way you walk?
Is scapular dyskinesis a normal or even beneficial adaptation? As mentioned above, professional overhead athletes exhibit differences in their scapulohumeral mechanics compared to non-athletes, and differences exist between different types of overhead athletes. Additionally, a systematic review by Burn et al. 2016 concluded that the prevalence of scapular dyskinesis in overhead athletes was 61% compared to 33% in non-overhead athletes. Might it be an advantageous adaptation like the changes seen in the throwing arm of a baseball pitcher?
Or does it even matter?
- Uhl et al. 2009 – “This study showed that scapular asymmetry in multiple planes, as determined by 3D kinematic analysis, is more prevalent in symptomatic subjects during humeral elevation in flexion but not in scaption. Asymmetry in 1 or more planes is seen with equal prevalence in both asymptomatic and symptomatic patients with a variety of shoulder pathologies.” Not very convincing.
- Tate et al. 2009 – “The presence of shoulder symptoms was not different between the normal and obvious dyskinesis volunteers.” The authors identified “no relationship between the presence of pain and scapular dyskinesis in these athletes.”
- Hickey et al. 2007 – 11 blinded physiotherapists (minimum 5 year experience) were only able to accurately classify a subject’s shoulders as asymptomatic or symptomatic 57.5% of the time (coin flip) and the overall agreement between examiners was quite low.
- Plummer et al. 2017 – “Our findings indicate that the occurrence of scapular dyskinesis is not influenced by the presence of shoulder pain. However, the rating of scapular dyskinesis does appear to be impacted by the clinician’s knowledge of the presence of shoulder pain in the involved shoulder.” If you know that a patient has a symptomatic shoulder (unblinded), you are more likely to label it as having scapular dyskinesis compared to a blinded observer. Essentially, we look for a fault that might not exist to confirm our biases.
The authors from the previous paper go on to state that “results from the current study indicate that the presence of scapular dyskinesis may not be a relevant impairment for those with shoulder pain and may represent normal movement variability.” So, scapular dyskinesis is quite normal and we cannot guess who has symptoms through observation alone, but does its presence increase your risk for injury?
Predicting Injuries
“An observed movement can predict who is at risk for injuries.” This is an argument we often hear, but hasn’t held up well in the literature for most body regions. “You might have asymptomatic scapular dyskinesis now, but you will go on to develop pain or injury later if you don’t fix it.” Is this really true? There are 7 prospective studies that I know of that can help answer this question. Let’s explore each one below.
- Kawasaki et al. 2012 – Asymptomatic scapular dyskinesis assessed preseason in high level, male rugby players was associated with developing shoulder discomfort during the season. The odds ratio was 3.6 so the individuals with asymptomatic scapular dyskinesis were 3.6 times more likely to develop shoulder pain during the season than those without scapular dyskinesis. However, the confidence interval did reach 1 so scapular dyskinesis had no impact on some participants (5/14 players with observable scapular dyskinesis did not report shoulder discomfort). 1 for 1 so far?
- Myers et al. 2013 – Scapular dyskinesis, assessed in the preseason, was not predictive of throwing-related upper extremity injuries in 246 varsity-level, male baseball players tracked over the course of 2 seasons. In fact, athletes defined as having normal scapular motion ended up having a higher injury rate. Swing and a miss? 1 for 2.
- Struyf et al. 2014 – Baseline data was taken for 113 recreational overhead athletes (males and females who played volleyball, badminton, tennis, baseball, and handball). They had follow-ups at 12 and 24 months. Despite assessing tilting, winging, forward shoulder posture, scapular upward rotation, and scapular dynamic control, the authors reported that “scapular characteristics could not predict the development of shoulder pain.” 1 for 3.
- Clarsen et al. 2014 – Elite, male handball players were assessed during preseason and tracked over the course of a season. Obvious scapular dyskinesis was significantly associated with what the authors defined as substantial shoulder problems (“shoulder problems leading to moderate or severe reductions in training volume or sporting performance, or a total inability to participate”). 2 for 4? We’ll return to this study in a moment.
- Shitara et al. 2017 – Scapular dyskinesis, assessed in the preseason, was not associated with upper extremity injuries in 105 male, high school baseball pitchers over the course of a season. 2 for 5.
- Andersson et al. 2018 – This paper was completed by the same authors as the Clarsen et al. article listed above. The title? “Risk factors for overuse shoulder injuries in a mixed-sex cohort of 329 elite handball players: previous findings could not be confirmed.” You can probably guess their findings. “In contrast to Clarsen et al, we did not find any association between scapular dyskinesis and shoulder injury.” 2 for 6 or do we exclude the previous tally now?
- Asker et al. 2020 – This study followed elite male and female adolescent handball players. Scapular dyskinesis was not associated with shoulder injuries in the female players. It was also not associated with shoulder injuries in the male players when assessed in flexion. However, the authors found an association when scapular dyskinesis was observed during abduction in the male players. I may be mistaken, but it seems they combined traumatic and non-traumatic shoulder injuries.
Note: I did not include the commonly cited Hickey et al. 2018 systematic review and meta-analysis because I thought the article by McKenna et al. 2012 was not representative of the topic at hand since the authors didn’t actually assess scapular dyskinesis.
So, what are we left with? Scapular dyskinesis was not associated with future injury in competitive baseball players and recreational overhead athletes. There are three studies on handball players, but the data seems conflicting. However, if you’re a high level, male rugby player, scapular dyskinesis seems to be associated with developing shoulder discomfort. I’d like to see this replicated, especially since I’m not sure I’d classify rugby as an overhead sport prone to “overuse” injuries.
Let’s assume scapular dyskinesis does predict future injury. How do we change it? More importantly, do we need to change it?
Traditional Rehabilitation
If we are identifying scapular dyskinesis as a relevant “dysfunction” of the shoulder complex, then we need to examine the literature that aims to correct it in individuals with pain.
- McClure et al. 2004 – Over the course of 6 weeks, subjects diagnosed with shoulder impingement syndrome were provided interventions aimed at (1) strengthening the rotator cuff and scapular stabilizers, (2) enhancing flexibility of the glenohumeral posterior capsule, pectoralis minor muscle, and upper thoracic spine, (3) improving upper-quarter postural awareness, and (4) enhancing patient understanding of environmental and workplace factors that place high loads on the shoulder. Despite no changes in scapular kinematics, participants had improvements in pain, satisfaction, and function after 6 weeks AND at a 6-month follow-up.
- Struyf et al. 2012 – The authors utilized a “scapular-focused” treatment in patients diagnosed with shoulder impingement syndrome. The subjects experienced a decrease in pain and had improvements in self-reported disability despite no change in scapular motor control, kinematics, or positioning.
- Mey et al. 2012 – Overhead athletes diagnosed with mild impingement symptoms had an improvement in symptoms and function with 6 weeks of scapular muscle rehabilitation exercises, but had no change in the timing of activation during arm elevation.
- Turgut et al. 2017 – 12 week randomized controlled trial assessing the effects of exercise on scapular kinematics, disability, and pain in individuals diagnosed with subacromial impingement. The control group received rotator cuff strengthening and stretching (“A”) while the intervention group received rotator cuff strengthening, stretching, and various closed and open chain scapular stabilization exercises (A+B). Both groups had improvements in self-reported pain and disability scores with no significant differences between the groups. The authors concluded that “adding scapular stabilization exercises to shoulder girdle stretching and strengthening exercises produced slightly better but arguably not clinically significant results regarding scapular kinematics after 6 and 12 weeks.” The study doesn’t mention blinding which is a concern considering the results of the Plummer et al. 2017 study.
I know what you might be thinking. “The scapular kinematics probably didn’t change because of the poor exercise selection or programming of the researchers.” Maybe. But does it really matter?
Based on these studies, it seems that scapular kinematics, or the scapulohumeral rhythm, does not need to change for shoulder symptoms or function to improve in individuals diagnosed with impingement (subacromial pain syndrome). If that’s the case, does changing the way the scapula moves need to be the goal of rehabilitation?
Probably not. We’ve already identified that we do not have a good working definition of “normal”. Plus, normal (whatever that is) likely exists on a spectrum based on the unique characteristics of the individual. Are they an overhead athlete? What type of overhead athlete? Adult or child? Male or female? Are we looking at the dominant or non-dominant side?
Scapular dyskinesis might also be an advantageous adaptation that develops over the course of an overhead athlete’s career. Do we really want to change it at the expense of potentially decreasing their performance?
Scapular dyskinesis is common in asymptomatic individuals and doesn’t seem to predict injury.
Is scapular dyskinesis (if we can define it) the cause [of pain] or the effect [of pain]?
Is there a potential harm in having a patient focus on changing their scapulohumeral rhythm? What if their symptoms improve, but their scapular kinematics do not and they become fearful or hypervigilant?
I honestly don’t have all the answers because the nature of pain, injury, and performance are incredibly complex, but I can frame how I would approach treatment in the next section. I don’t want you to think that I’m a nihilist who thinks nothing matters.
Practical Recommendations
First and foremost, let it be known that I think we should still assess for scapular anomalies that might require further diagnostic testing from the appropriate healthcare provider, such as an insult to the brachial plexus, dorsal scapular nerve, spinal accessory nerve, or long thoracic nerve. This would likely be something that really stands out and may fit both the subjective history (preceded by a specific mechanism of injury) and objective findings (noticeable weakness, atrophy, range of motion loss, etc.). However, conservative management may still be the first line of treatment in many cases regardless of the diagnosis.
Do I think exercise selection and dosage matter? Yes, absolutely. I just don’t think exercises should be prescribed with the intention of changing how the scapula moves.
What should we do instead? Find out what matters to the patient. What are their goals and what is limiting them from accomplishing those goals? Pain? Weakness? Range of motion limitations? Fear? I’m not saying that any of these are causal in nature either. I’m also not saying the reason patients report improvements in symptoms is solely because their strength or range of motion improves. I understand that pain is complex and multi-factorial. Nevertheless, we can try to analyze the demands of the task or, when appropriate, compare to their contralateral side, and attempt to improve their capacity to tolerate the necessary stressors.
How might this look? Well, many “scapular” rehabilitation programs are aimed at strengthening the lower trapezius and serratus anterior. Rather than overemphasizing a particular muscle, why not consider the relevant movements that are challenging for the patient. Let’s use a sample list of questions that we can ask the patient (italics for theoretical answers):
- Do you have difficulty with pushing or pulling movements? Pushing.
- Do you have difficulty with vertical/overhead or horizontal pushing movements?
- Vertical
- Weightbearing or non-weightbearing?
- Non-weightbearing
- Weightbearing or non-weightbearing?
- Horizontal
- Weightbearing or non-weightbearing?
- Weightbearing
- Weightbearing or non-weightbearing?
- Vertical
Okay, so we’ve identified that the patient has trouble with non-weightbearing vertical and weightbearing horizontal pressing movements. How do we address that?
Weightbearing Horizontal Pressing Progression:
Non-Weightbearing Vertical Pressing Progression:
Yes, I understand that this isn’t perfect. Just let me explain. As I mentioned above, we often obsess over the serratus anterior. Well, the weightbearing horizontal pressing progression is an excellent way to strengthen the serratus anterior without making it the sole focus. The movement is also challenging the pecs, triceps, deltoids, and rotator cuff. You can get serious strength gains from a band-resisted push up. Plus, you can easily turn this movement into a downward dog, toe tap, plank with rotation, etc. if you wanted to transition to overhead or single arm.
The non-weightbearing progression doesn’t actually have any vertical pressing, though. I know. You could just scale an overhead press. However, I know that athletes don’t care about vertical pressing – they care about being able to play their sport (throwing a ball, spiking a volleyball, etc.). Once again, this is just one random, easy progression to eventually get overhead while increasing the capacity of the entire shoulder (and more than sufficiently trains the lower trapezius).
What does the person want to do? What’s their current capacity? Fill in the gaps. Then follow the sage words of Louis Gifford: start easy, build slowly (relatively!).