Do you have shoulder pain when sleeping on your side or while reaching out, overhead, or behind your back?
In this blog, I’m going to each you everything you need to know about rotator cuff tears, discuss whether or not surgery is always necessary, and provide you with a comprehensive rehab program.
The rotator cuff consists of 4 separate muscles that attach from the scapula, or shoulder blade, to the humerus, or arm bone. These four muscles are the subscapularis on the front of the shoulder blade, the supraspinatus on the top, and the infraspinatus and teres minor on the back.
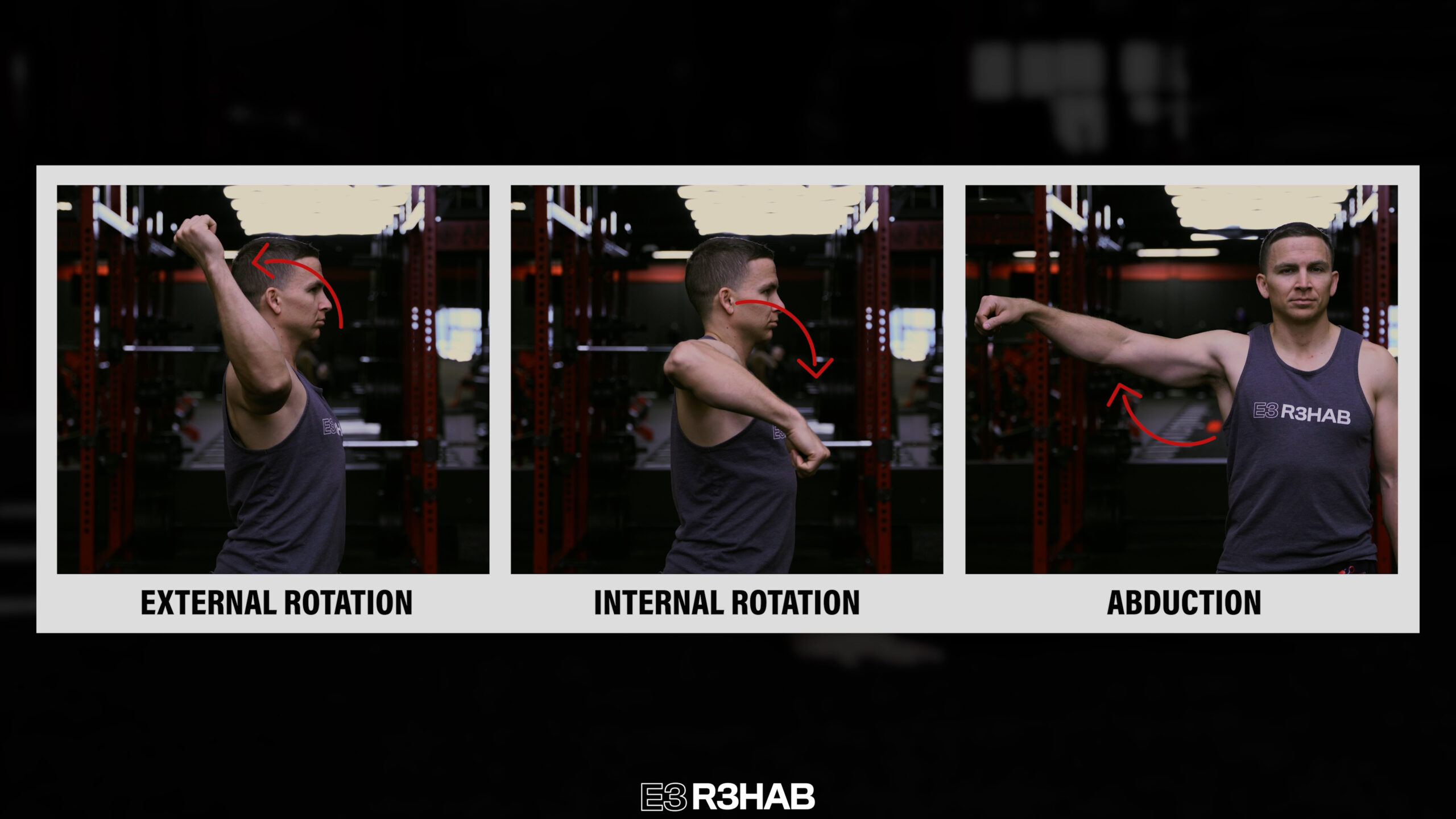
Although these muscles contribute to individual joint actions of the shoulder, such as external rotation, internal rotation, and abduction, they are most well known for their role in providing “dynamic stability,” which means they actually help control and support the shoulder with every movement.
This is largely due to the fact that they are somewhat interconnected, surround most of the shoulder, and blend together with the joint capsule.
Impingement, Tendinitis, and Rotator Cuff Tears (Oh My!)
When it comes to the shoulder, pain can often be divided into 3 broad categories:
The Stiff Shoulder, like Frozen Shoulder or Adhesive Capsulitis
The Unstable Shoulder, which relates to a history of dislocations or subluxations
The Weak & Painful Shoulder, which is the topic of this blog
Under this umbrella of the weak and painful shoulder are the following diagnoses (among others):
Shoulder Impingement
Subacromial Pain Syndrome
Rotator Cuff Tendinitis, Tendinosis, or Tendinopathy
Rotator Cuff Related Shoulder Pain
Rotator Cuff Tears
Let me explain.
It’s often believed that imaging, injections, and surgeryare required for these conditions, but in general, exercise therapy is the first-line recommendation because symptoms related to any of these diagnoses likely have more to do with current tissue sensitivity from sudden or gradual changes in activity and your overall health as opposed to compression of structures, excessive local inflammation, or new tears of your rotator cuff.
A systematic review by Teunis et al stated the following: “The prevalence of rotator cuff abnormalities in asymptomatic people is high enough for degeneration of the rotator cuff to be considered a common aspect of normal human aging and to make it difficult to determine when an abnormality is new (e.g., after a dislocation) or is the cause of symptoms.”
Am I talking about partial-thickness tears or full-thickness tears?
Both.
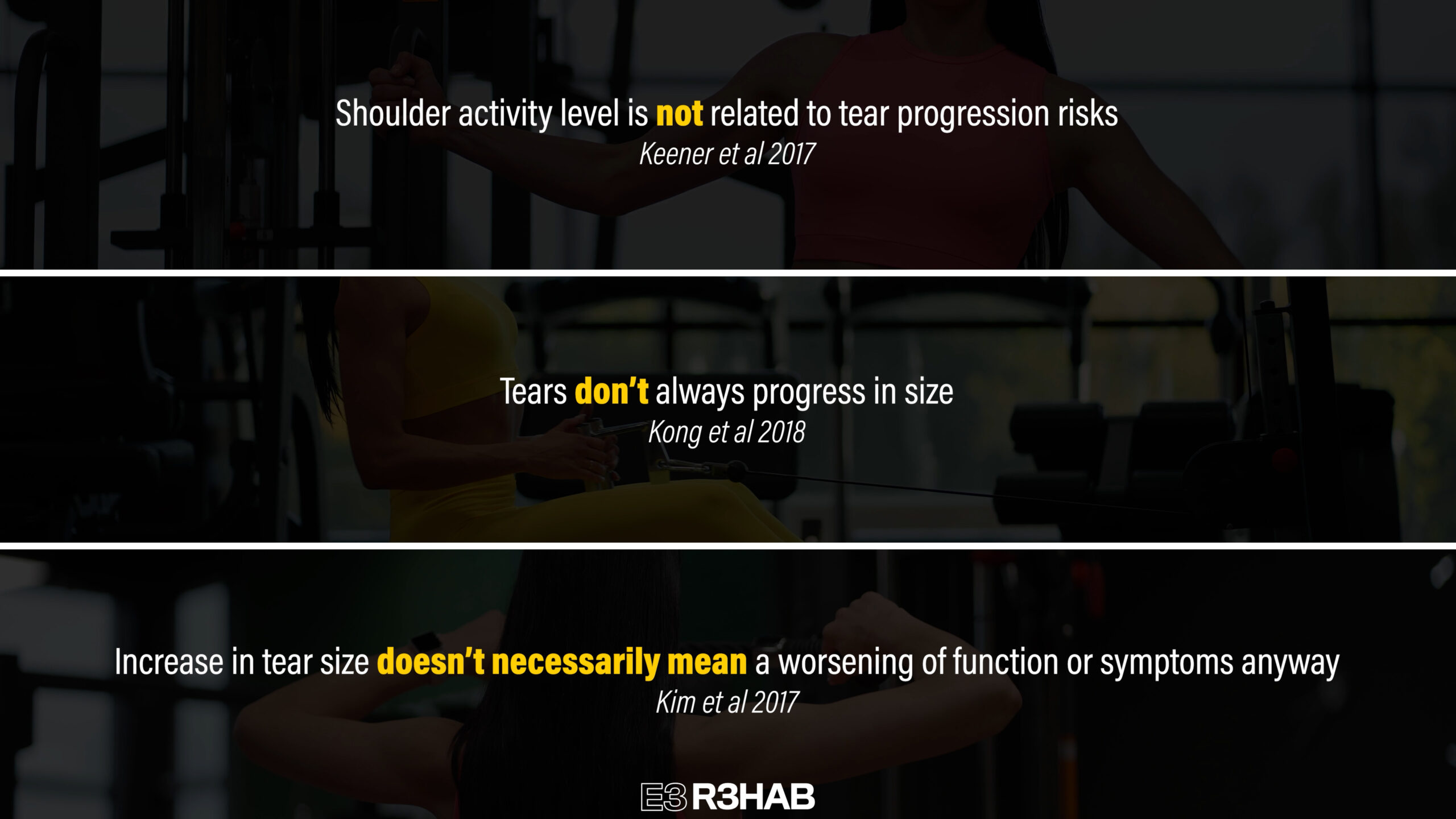
A recent study by Hinsley et al found that 48.4% of full-thickness tears were asymptomatic in the population studied.
Another recent systematic review and meta-analysis by Fahy et al concluded that, “Based on the available evidence exercise is as effective as surgery for improving quality of life, disability and pain for large to massive rotator cuff tears…”
Understanding and Monitoring Pain
How is this possible?
Rotator cuff tears are often thought to be like a rope cut in half, but they’re more similar to a hole in a piece of cloth due to their interconnecting nature that I discussed at the beginning.
The cloth still works fine, which is why many people don’t experience pain or changes in function despite having a rotator cuff tear.
Does that mean surgery is never indicated? No. You should always consult with your medical doctor before making any decisions, especially if trauma was involved.
As I mentioned earlier, symptoms are more about the shoulder being currently sensitive to certain positions, movements, and exercises rather than the occurrence of irreparable damage. It’s actually acceptable to have some discomfort during rehab if it’s tolerable for you and you’re slowly progressing toward your goals over time. You’re not hurting yourself.
The goal of rehab, at least for this blog, is pretty simple – it’s to temporarily modify any aggravating activities, improve your overall health with lifestyle modifications and exercise where possible, and incorporate an exercise routine that’s manageable, tolerable, and addresses any of your deficits in strength, range of motion, confidence, etc. Sanford 2017, Powell 2021, Powell 2023, Clausen 2023
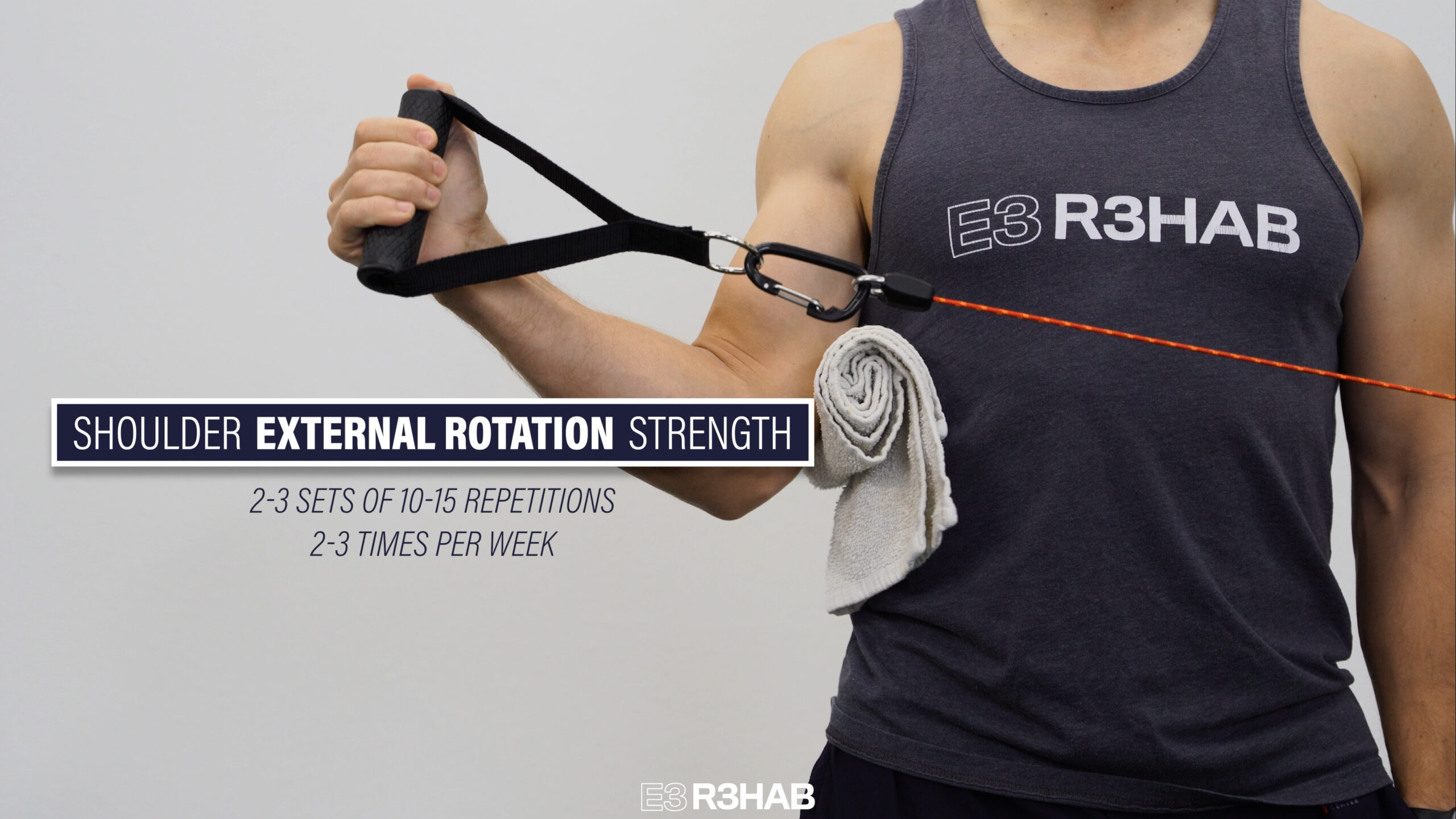
Shoulder External Rotation Strength
The first group of exercises relates to shoulder external rotation strengthening, which is often associated with rotator cuff strengthening.
Here are 3 options to choose from:
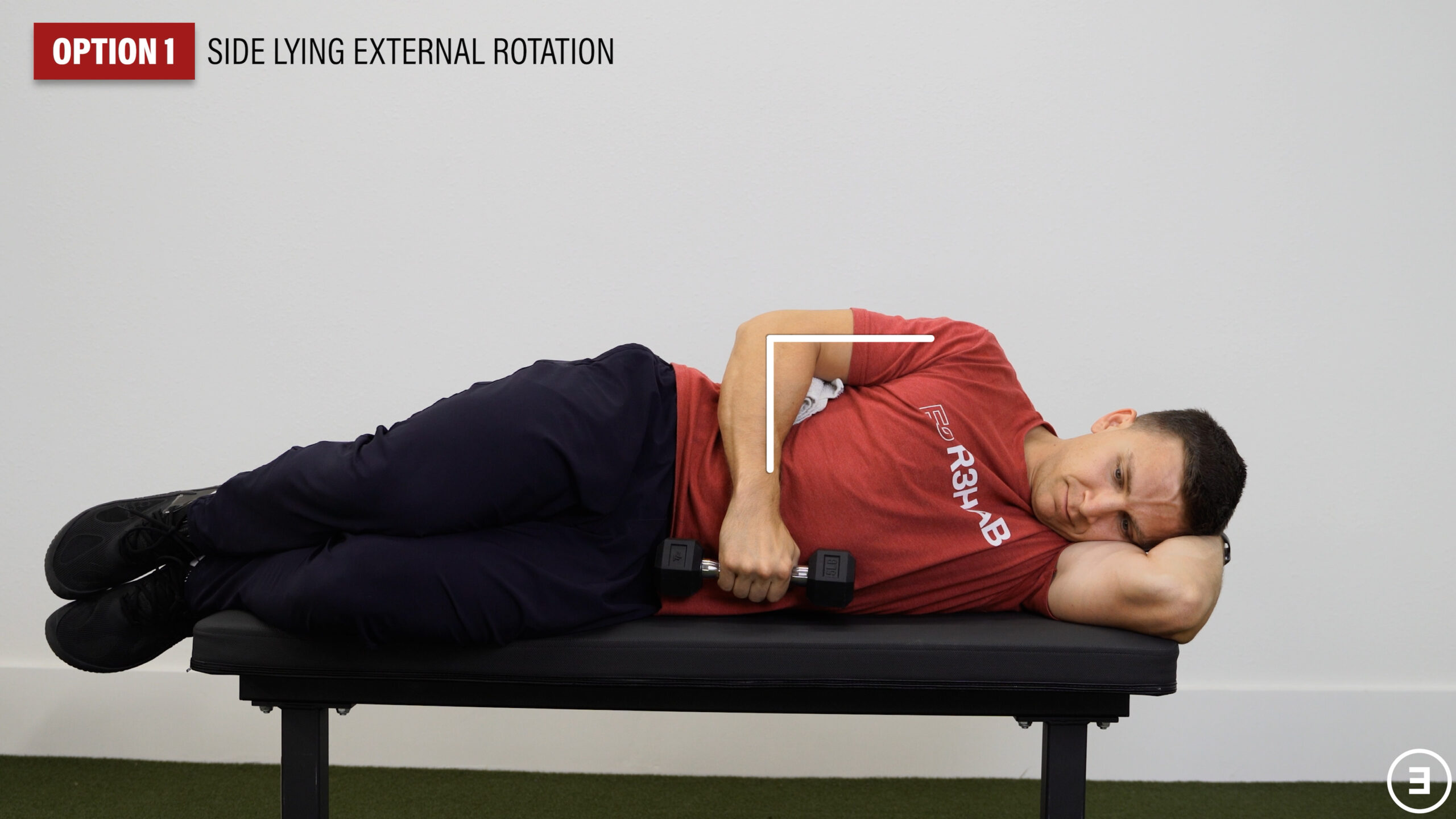
Option 1: Side Lying External Rotation – Place your top arm at your side with your elbow bent to 90° while holding a weight in your hand. Rotate your arm outward while keeping your arm at your side. Lower back to your stomach and repeat.
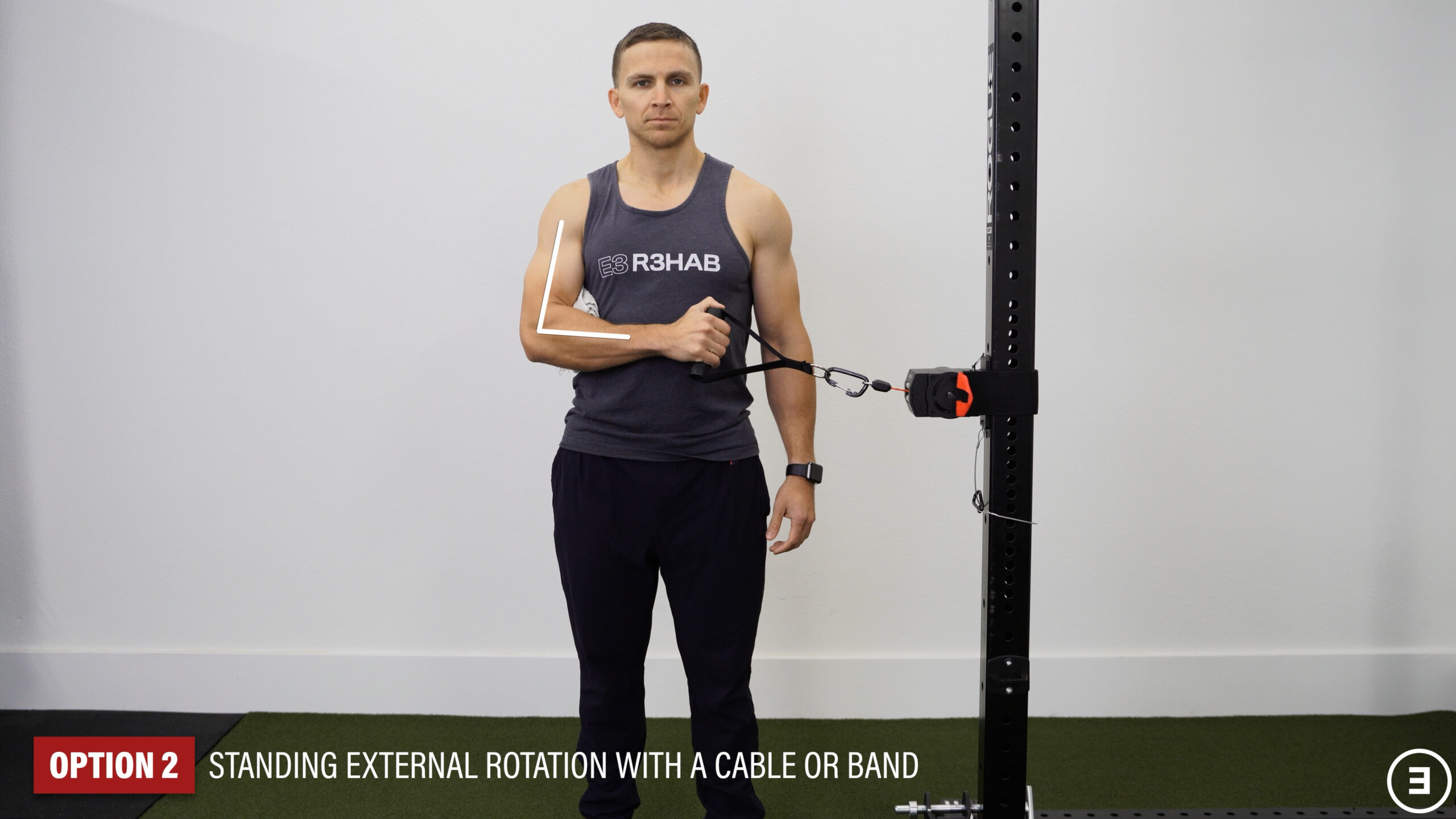
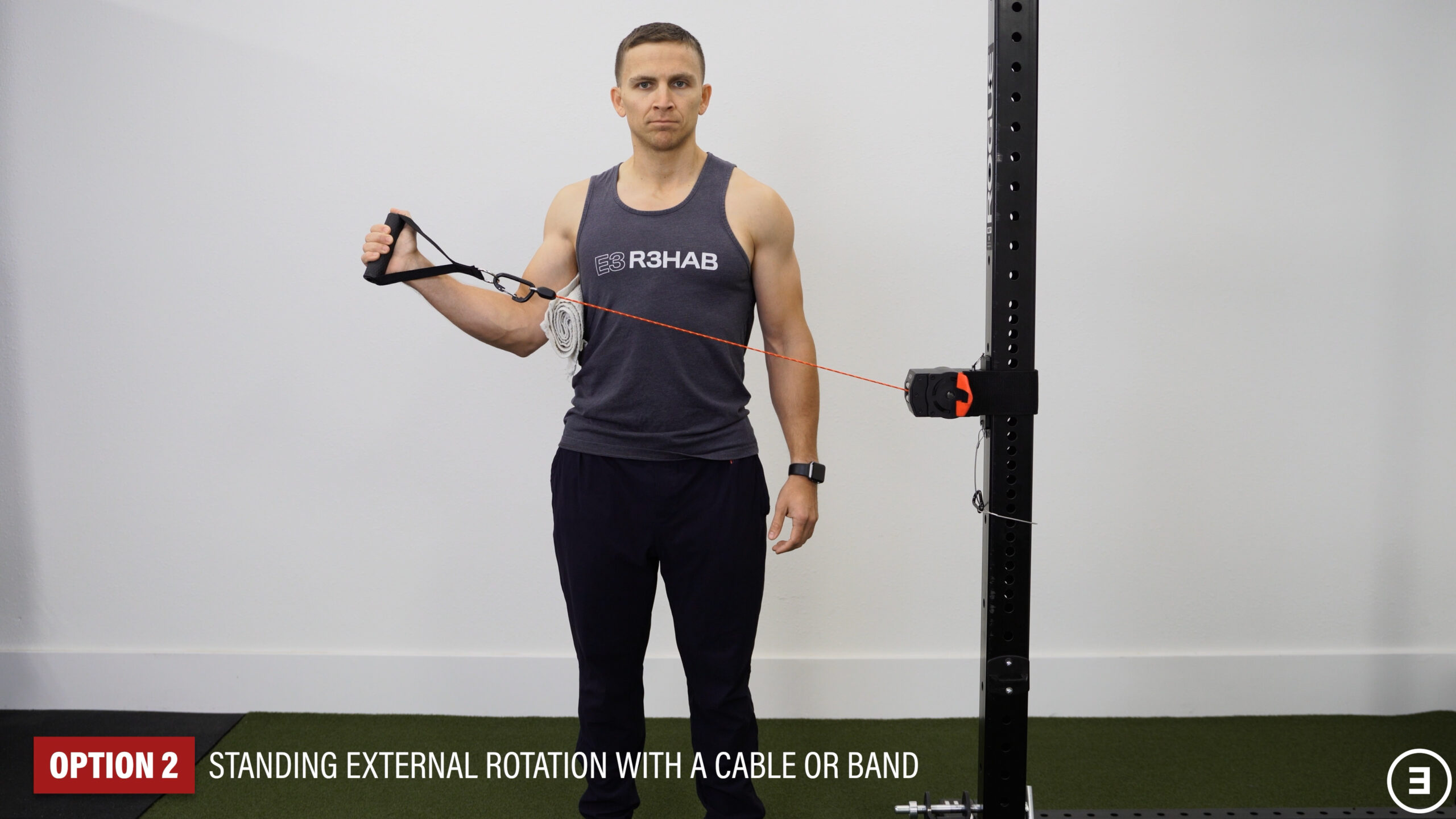
Option 2: Standing External Rotation with a Cable or Band – With your elbow bent to 90° and pinned at your side, rotate your arm outward. Slowly control the motion back to the start and repeat.
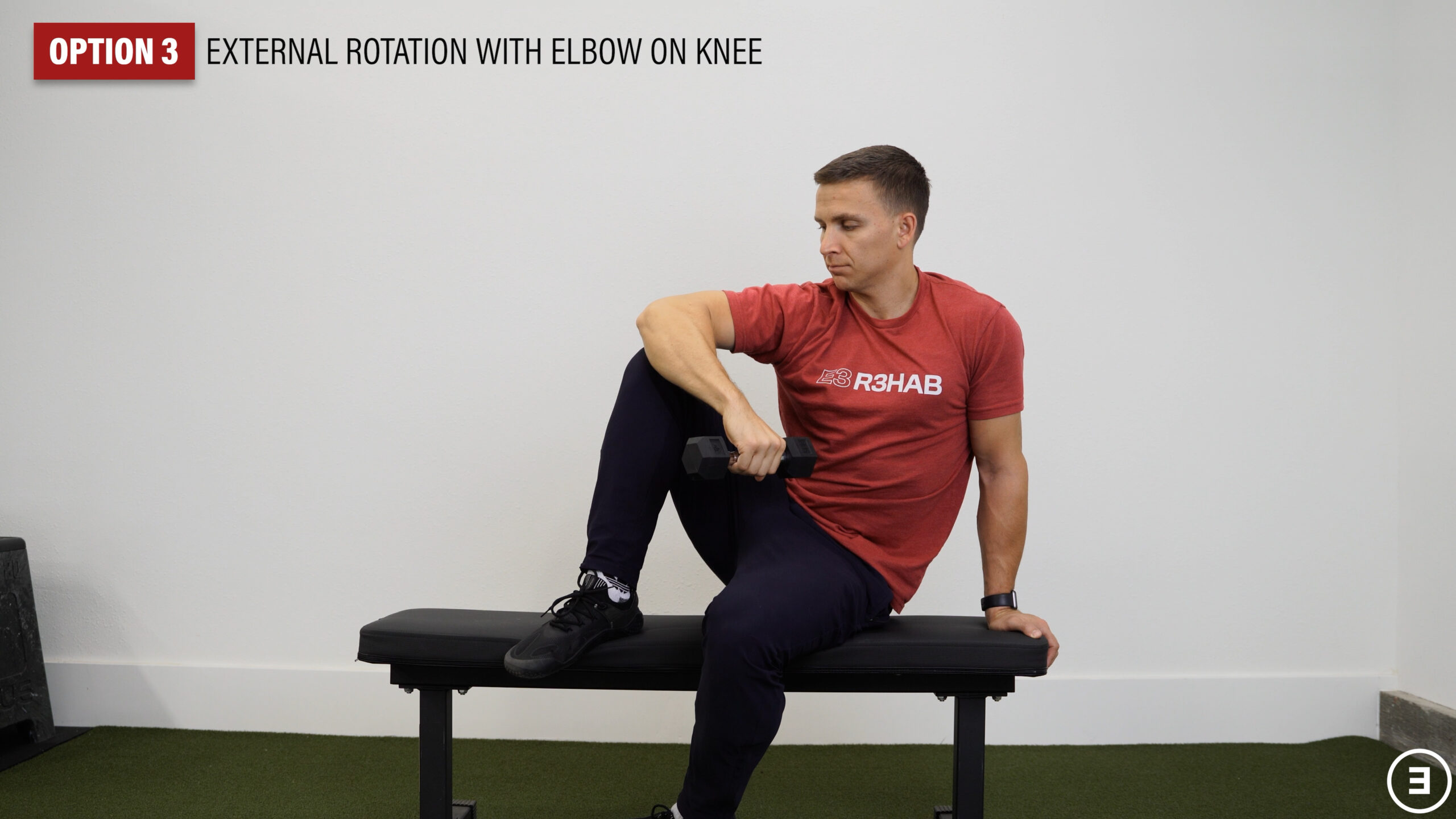
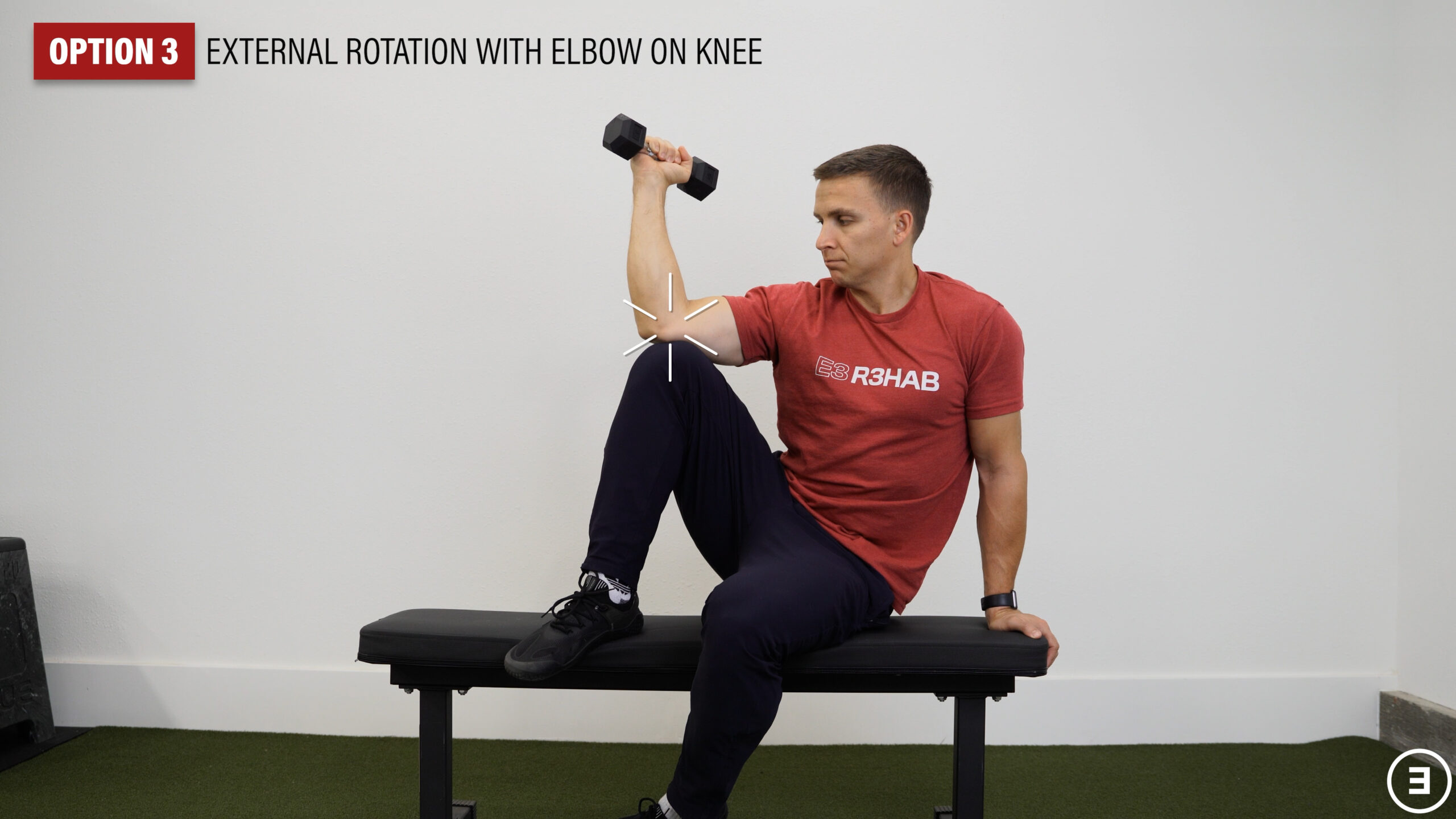
Option 3: External Rotation with Elbow on Knee – Sit with your elbow supported on your knee and a weight in your hand. Slowly lower the weight, rotating your arm inward as far as possible without letting your shoulder roll forward. Then, rotate back to the starting position.
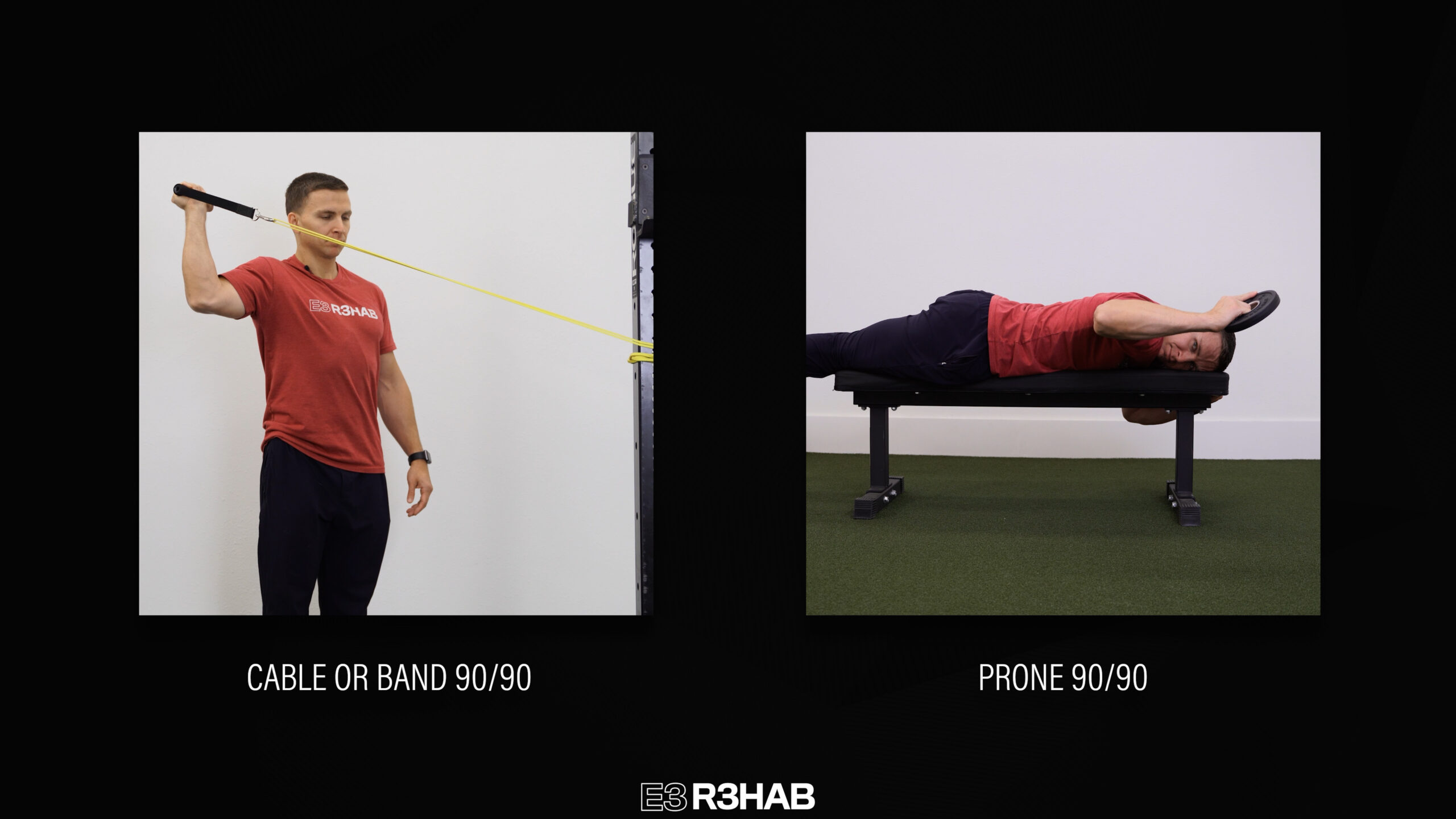
If you want to progress these exercises, you can perform them in what’s known as the “90/90 position”, in which the shoulder and elbow are bent to 90 degree angles.
If you’re standing, use a cable or band. If you’re lying on your stomach, use a weight.
Any of these exercises can be done for 2-3 sets of 10-15 repetitions, 2-3 times per week.
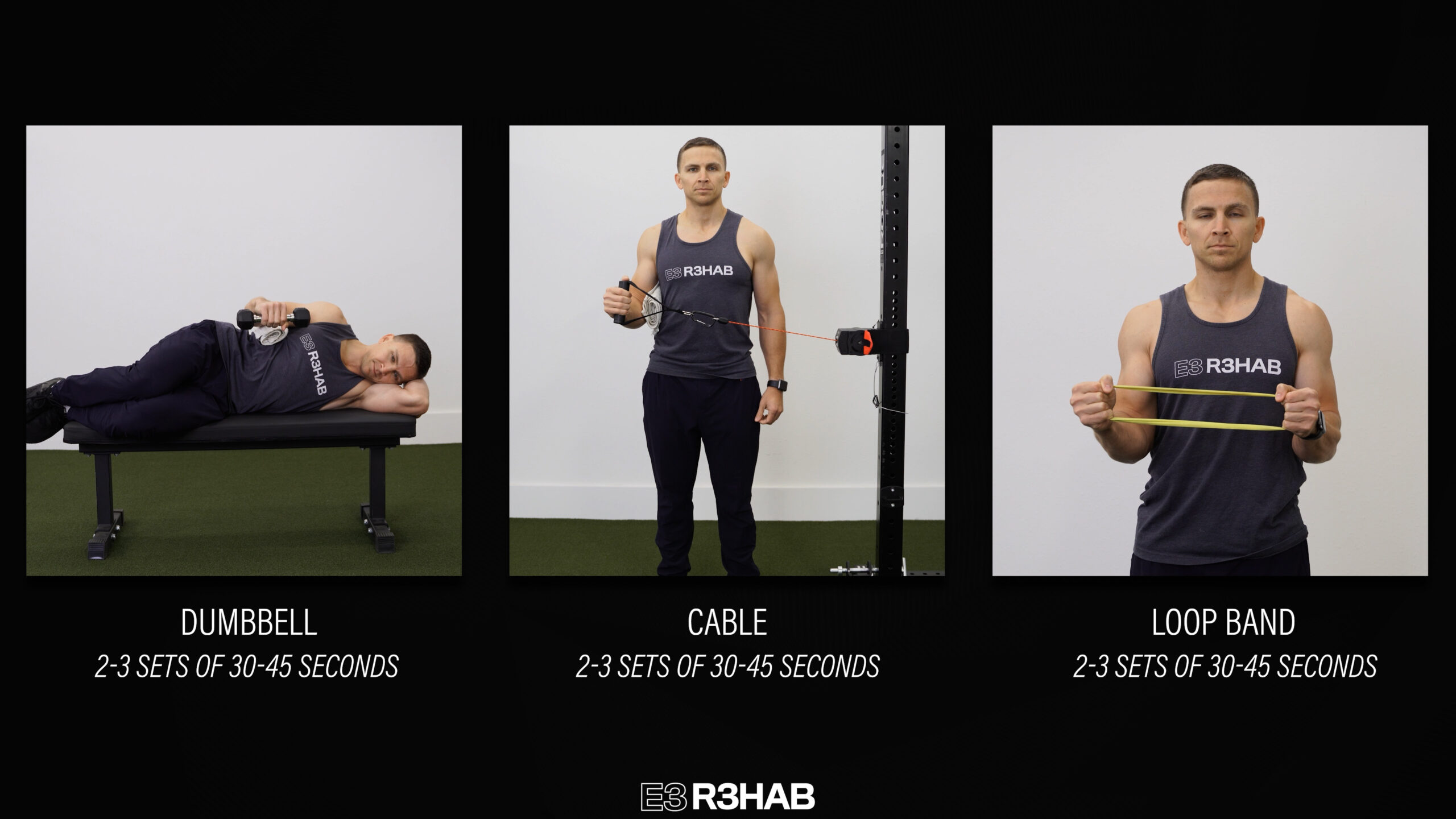
If you need an easier external rotation strengthening option, try an isometric variation, which is just a static hold.
You can do this in side lying by holding your arm in place or while standing with a ribbon band, cable, or loop band.
Any of these options can be done for 2-3 sets of 30-45 seconds.
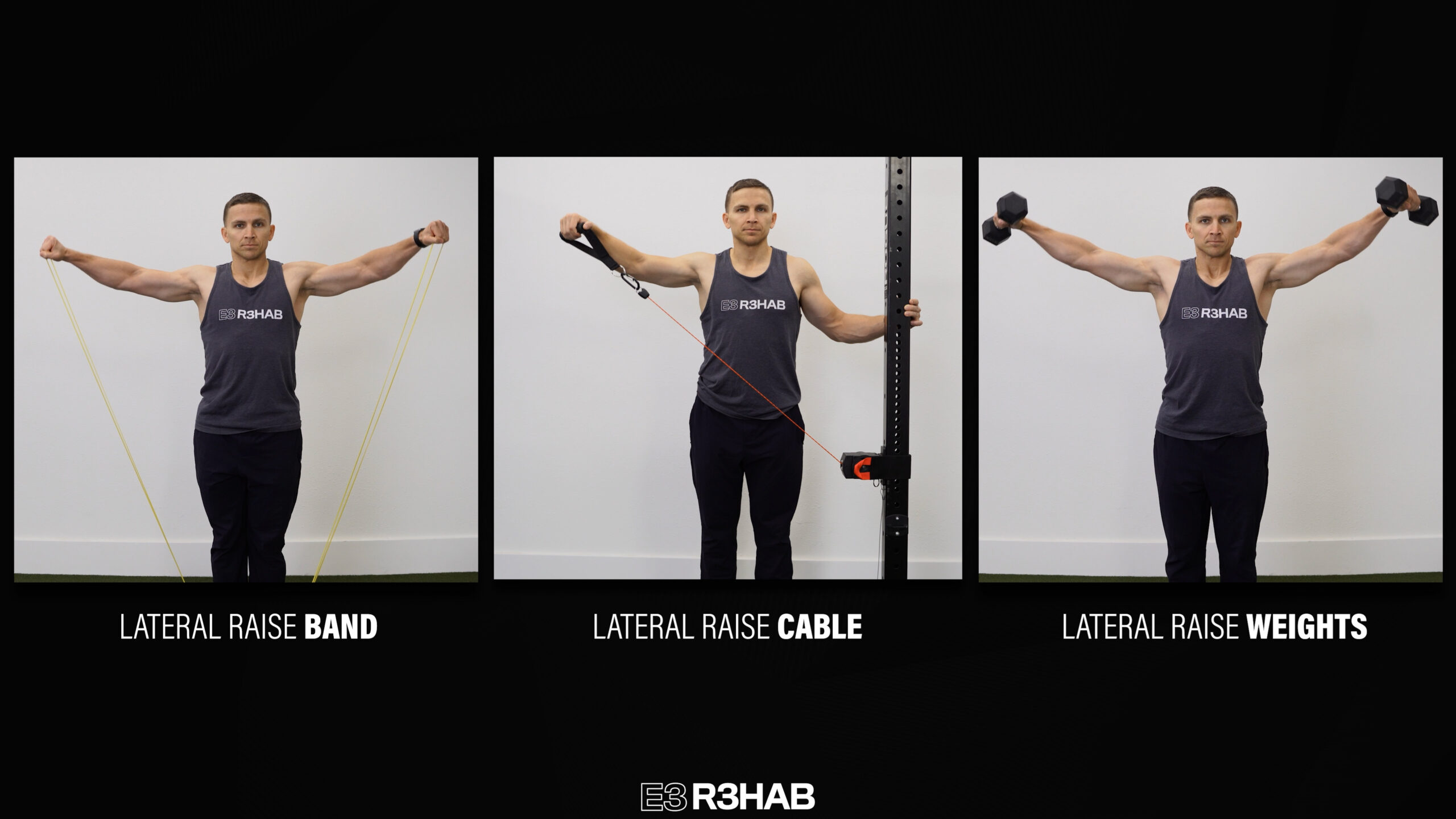
Shoulder Abduction Strength
The next group of strengthening exercises relates to shoulder abduction.
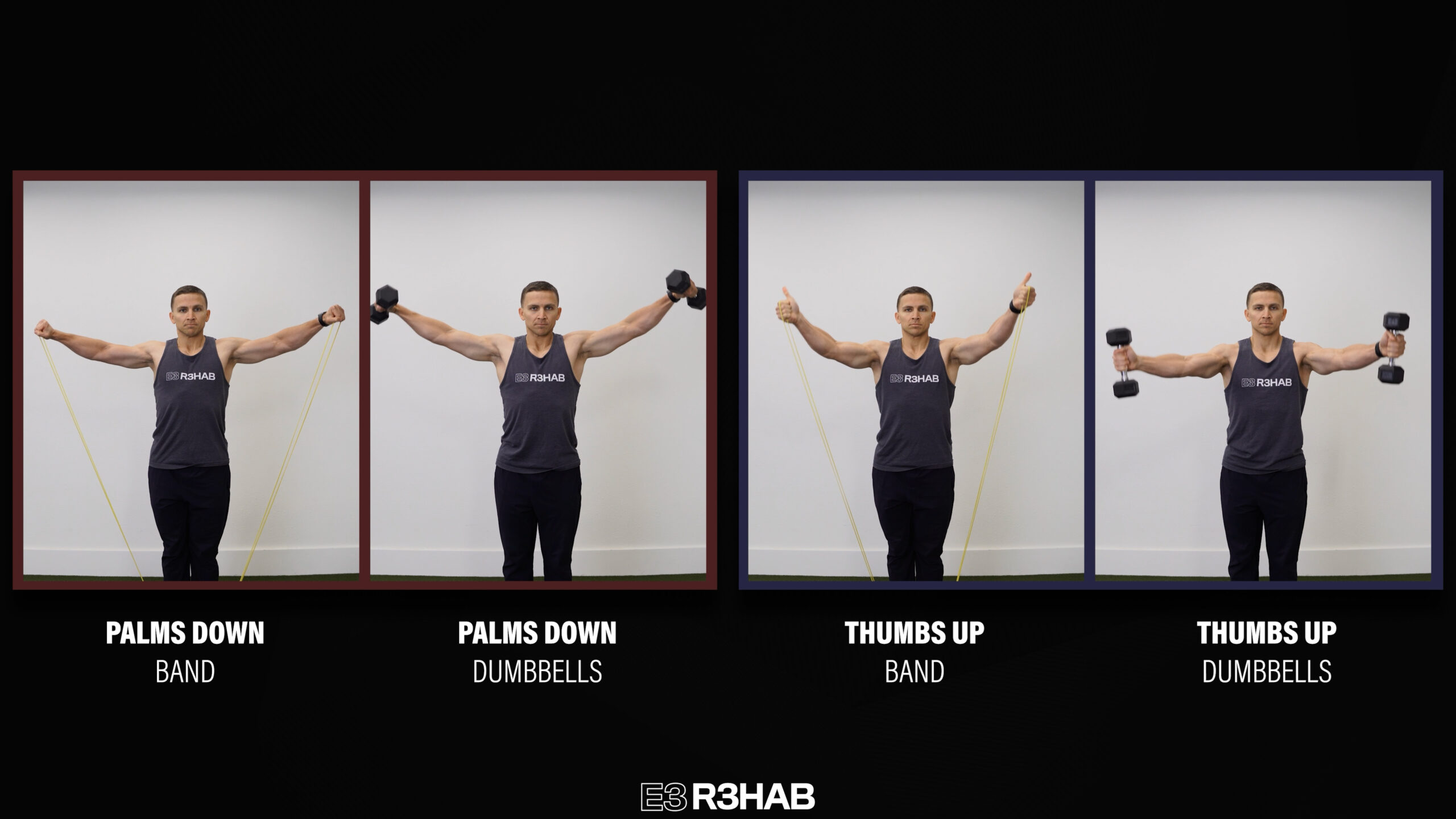
The main option is a lateral raise. Raise your arms up to about shoulder height using a band, cable, or weights.
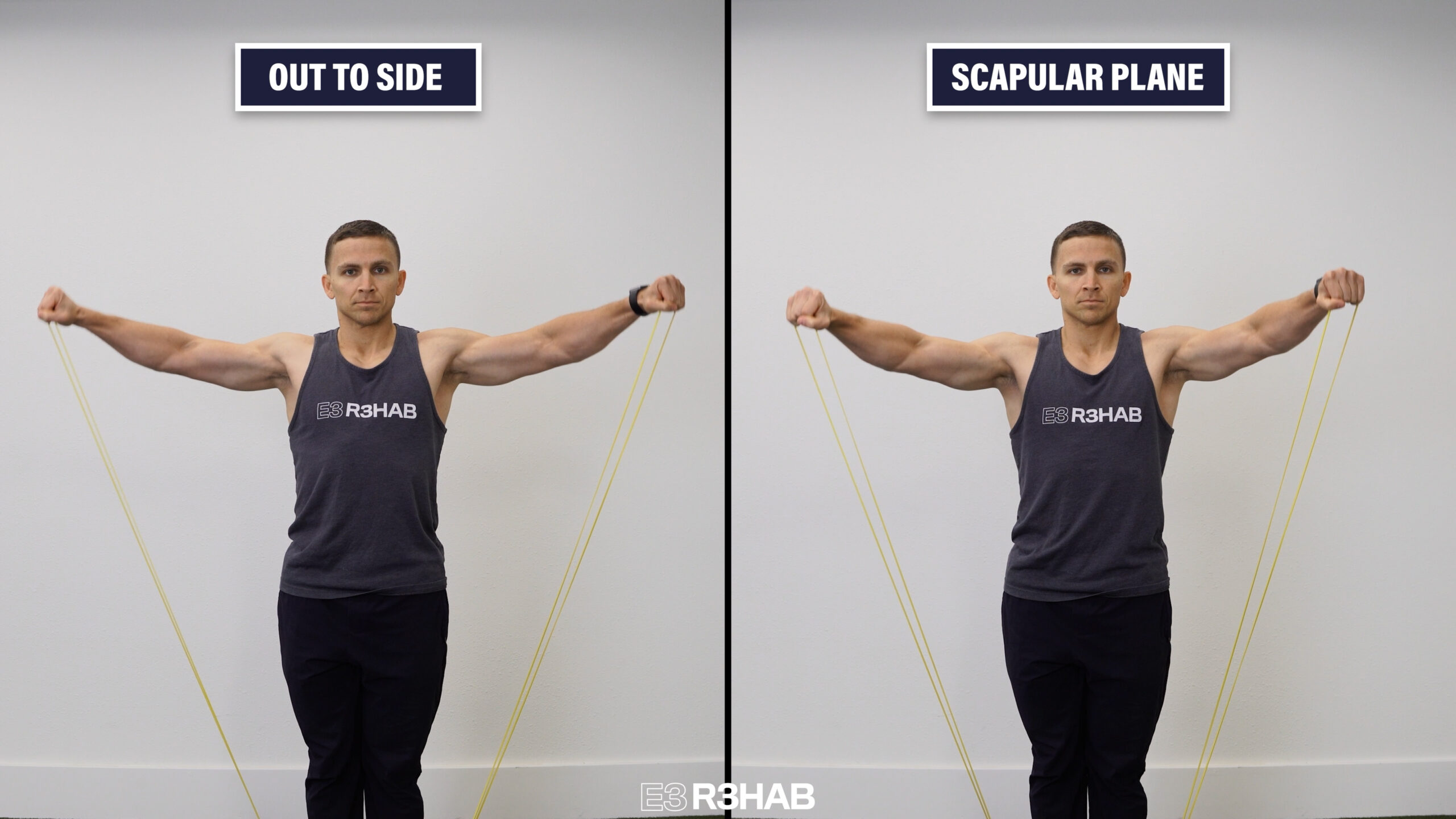
Your arms can be directly out to your side or in what’s referred to as the scapular plane, which is about a 30-45 degree angle in front of you.
Your palms can be facing down or you can turn your thumbs up toward the ceiling. If you have your thumbs up toward the ceiling, you can raise your arms slightly above shoulder height.
Since shoulder abduction is often problematic in the early phase of rehab, an isometric variation can be performed by spreading a loop band or pushing into a wall. You can also shorten the range of motion of the previous options.
Once again, exercises can be completed for 2-3 sets of 10-15 repetitions or 30-45 second holds, 2-3 times per week.
Posterior Shoulder Strength
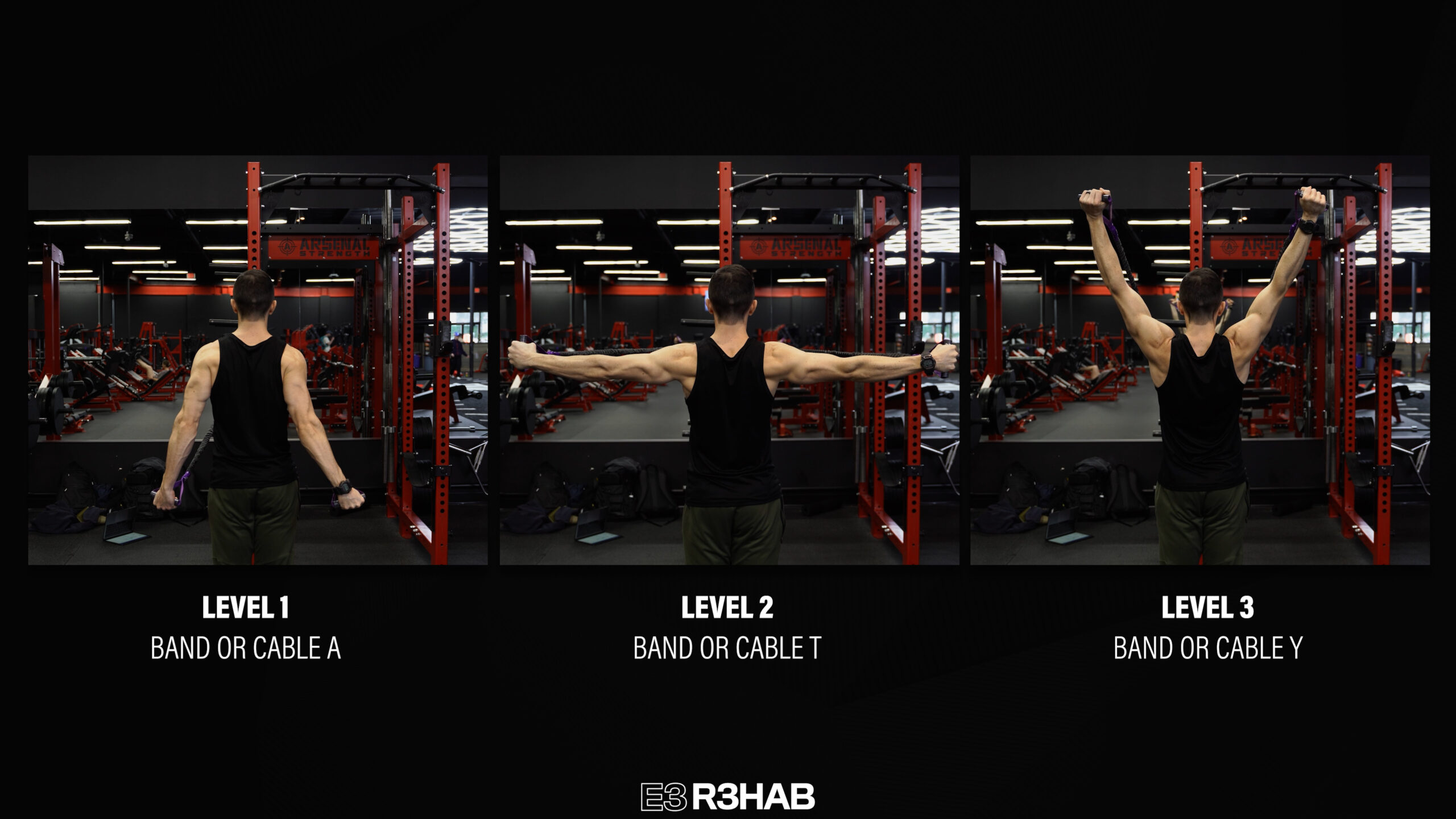
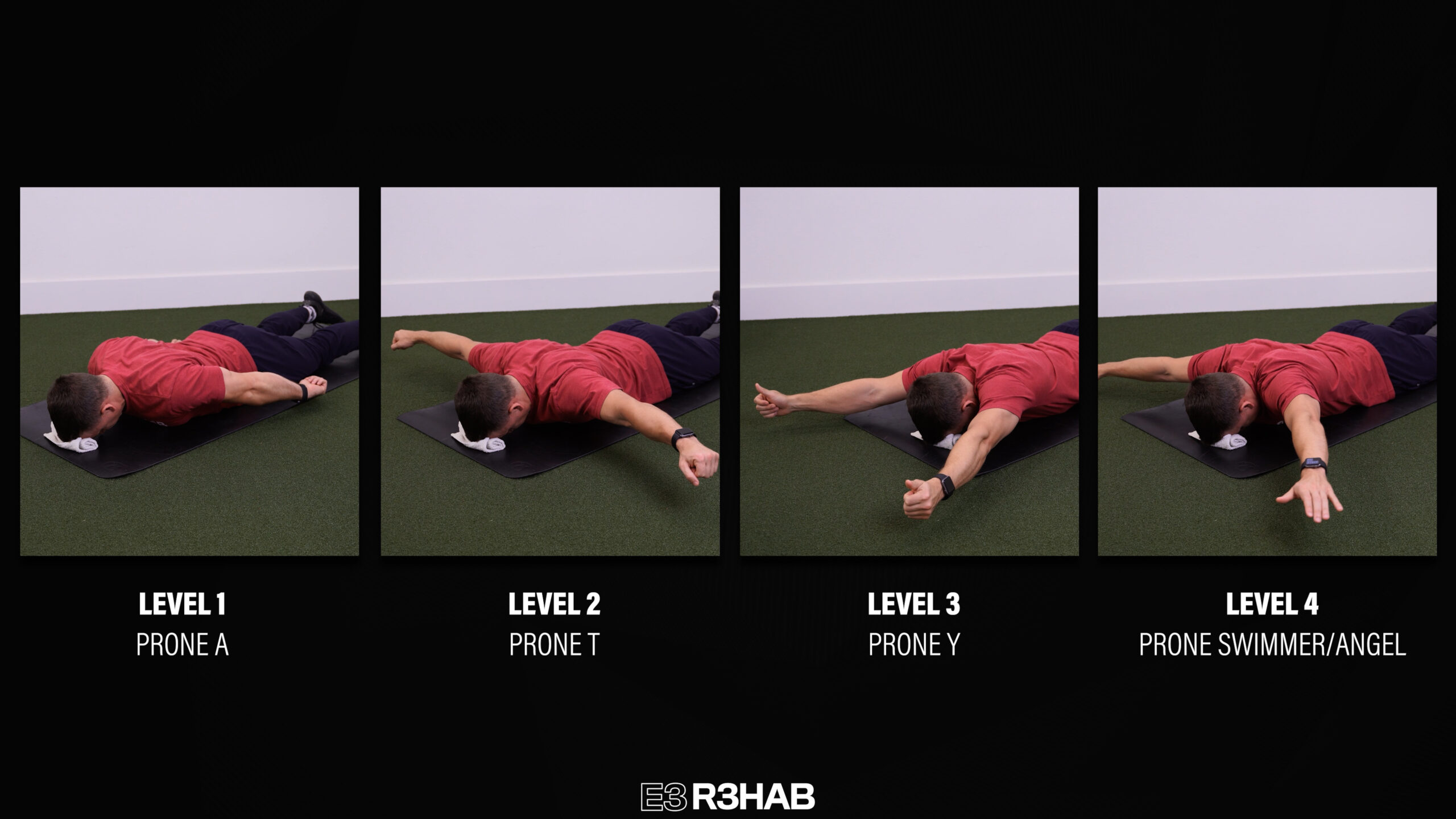
The third category of exercises is all about strengthening the back of the shoulders and upper back. The goal is to begin with your arms down by your side and gradually progress overhead. You probably know these as As, Ts, and Ys.
There are 3 options:
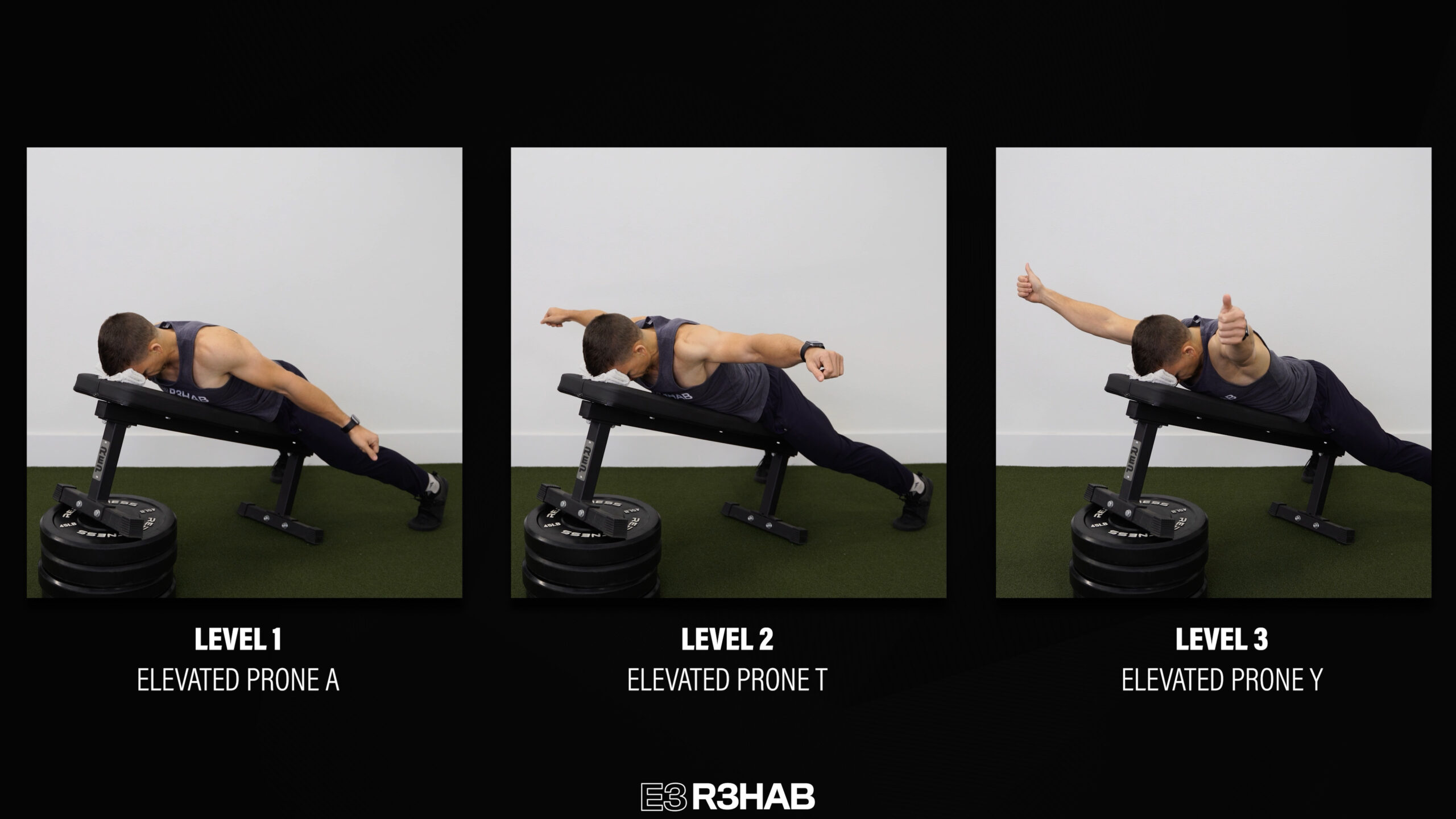
Option 1 requires you to lie face down on an incline bench or elevated surface so your hands don’t hit the ground.
Start with As, progress to Ts, and eventually try Ys. At the top of the Ts and Ys, your palms can be facing the ground or you can point your thumbs up toward the ceiling. Add resistance in the form of cuff weights, dumbbells, or weight plates when you’re ready.
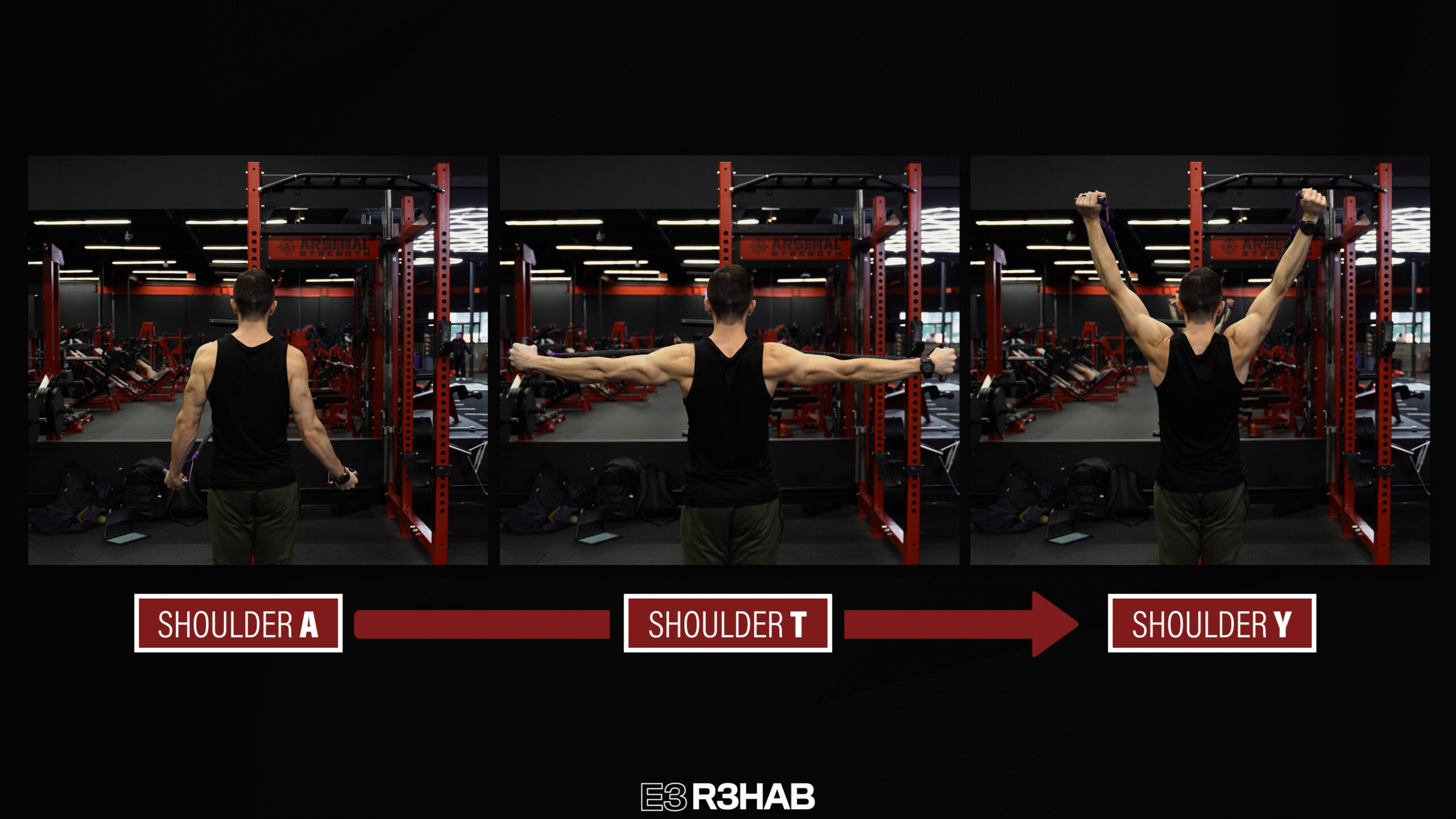
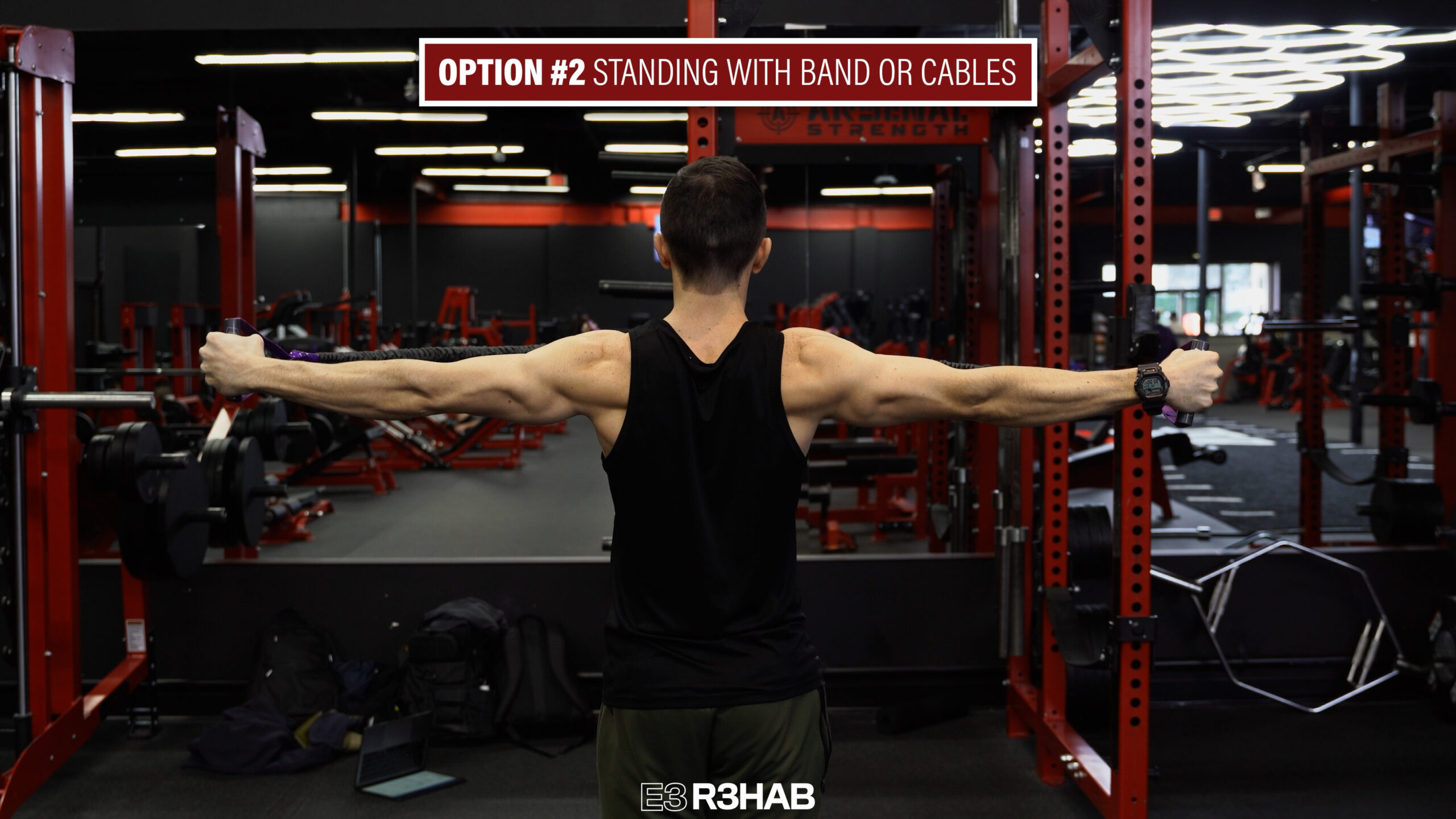
Option 2 is performed in standing with cables or bands.
For As, you’ll start high and pull low. For Ts, you’ll work at shoulder height. For Ys, you’ll start low and pull high. In addition to repetitions, you can perform isometrics at different ranges of motion.
Option 3 is performed on the ground.
Although you can perform repetitions, isometrics are probably preferred since you’re moving your shoulders through very little range of motion. You can also perform prone swimmers or angels in this position. If you want to challenge your shoulder extension and internal rotation, you can start the prone angels with your hands behind your back.
Keeping things simple, exercises can be done for 2-3 sets of 10-15 repetitions or 30-45 second holds, 2-3 times per week. The prone angels are more time consuming, so you can use a timer or do less than 10 repetitions.
Weight Bearing Strength
Since the rotator cuff doesn’t just contribute to isolated shoulder movements, the next strengthening category involves weight bearing.
The standard option here is a plank on your hands or forearms. Squeeze your glutes, keep your low back relatively flat, and think about pushing the floor away from you to work on protraction of your shoulder blades.
To make planks easier, perform them on your knees or elevate your hands on a bench, countertop, or even against the wall if needed.
There are an infinite number of ways to make planks harder, so here are 3 examples:
Long Lever Plank – While maintaining the same technique, perform a plank with your forearms higher up.
Dolphin Pose – Set up in your forearm plank, take a deep breath out, and press the floor away from you as you bring your hips toward the ceiling. Take a breath in, return to the starting position, and repeat.
Shoulder Taps – Set up in your tall plank, spread your feet, and tap your opposite shoulder in alternating fashion while minimizing movement from your trunk. Be sure to continue thinking about pushing the floor away from you with the hand that’s on the ground.
These can be performed for 2-3 sets of 30-60 seconds, 2-3 times per week.
Compound Pushing and Pulling Exercises
Similarly, compound pushing and pulling exercises can be a component of rehab if they’re necessary for your goals.
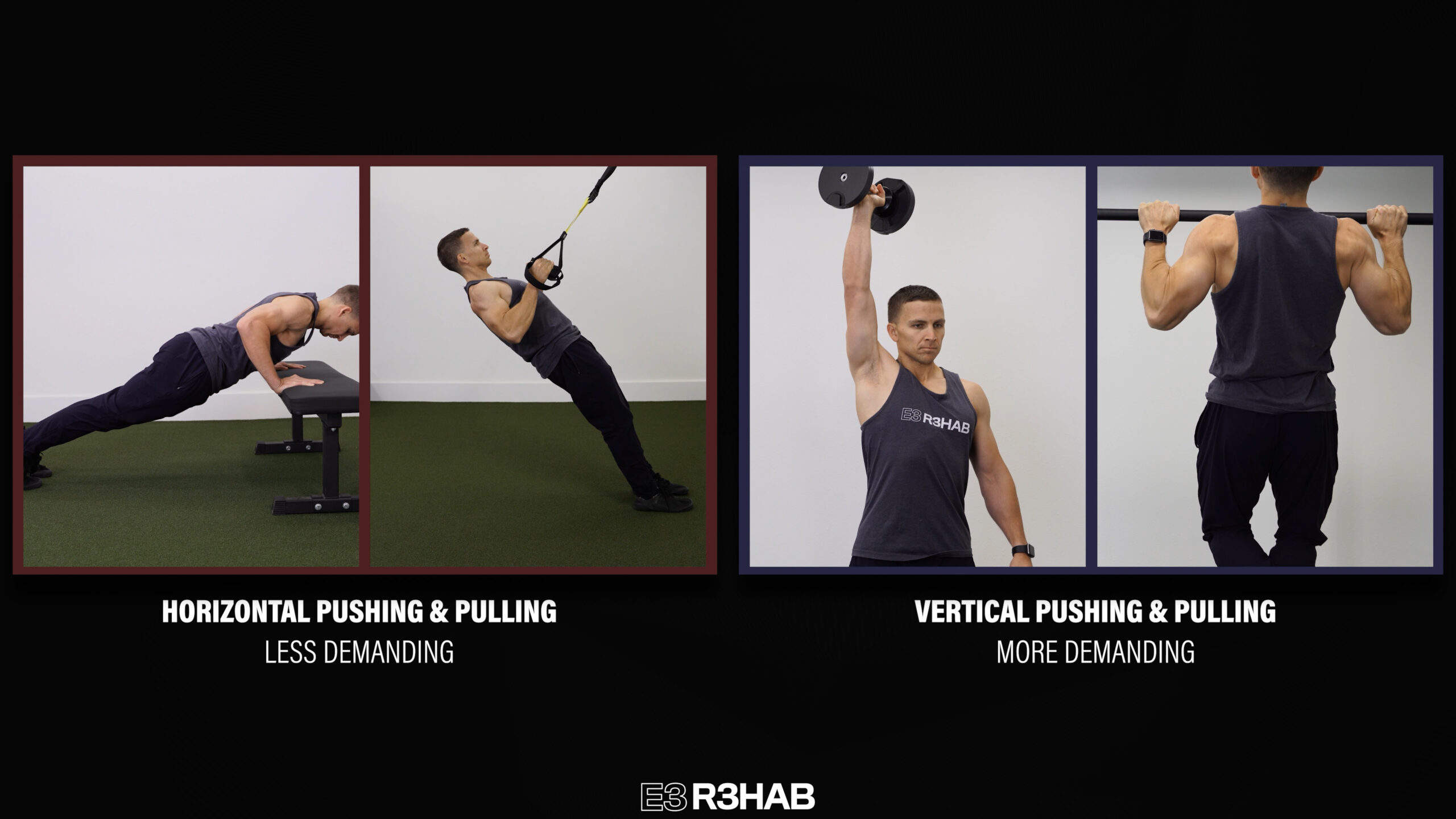
One of the best options for compound pushing exercises initially would be a push-up, which can be made easier by elevating your hands and harder by elevating your feet or increasing the range of motion.
Inverted rows and TRX rows are also good options because you can change your body position to make the exercise easier or harder.
For example, being more upright will make the exercise less challenging while being more horizontal will make the exercise more challenging.
A simple rule of thumb is that horizontal pushing and pulling movements are going to be less demanding on the shoulder than vertical pushing and pulling movements.
Other than that, there are so many variables you can adjust: volume, intensity, range of motion, tempo, exercise selection, etc.
Shoulder Flexion Range of Motion
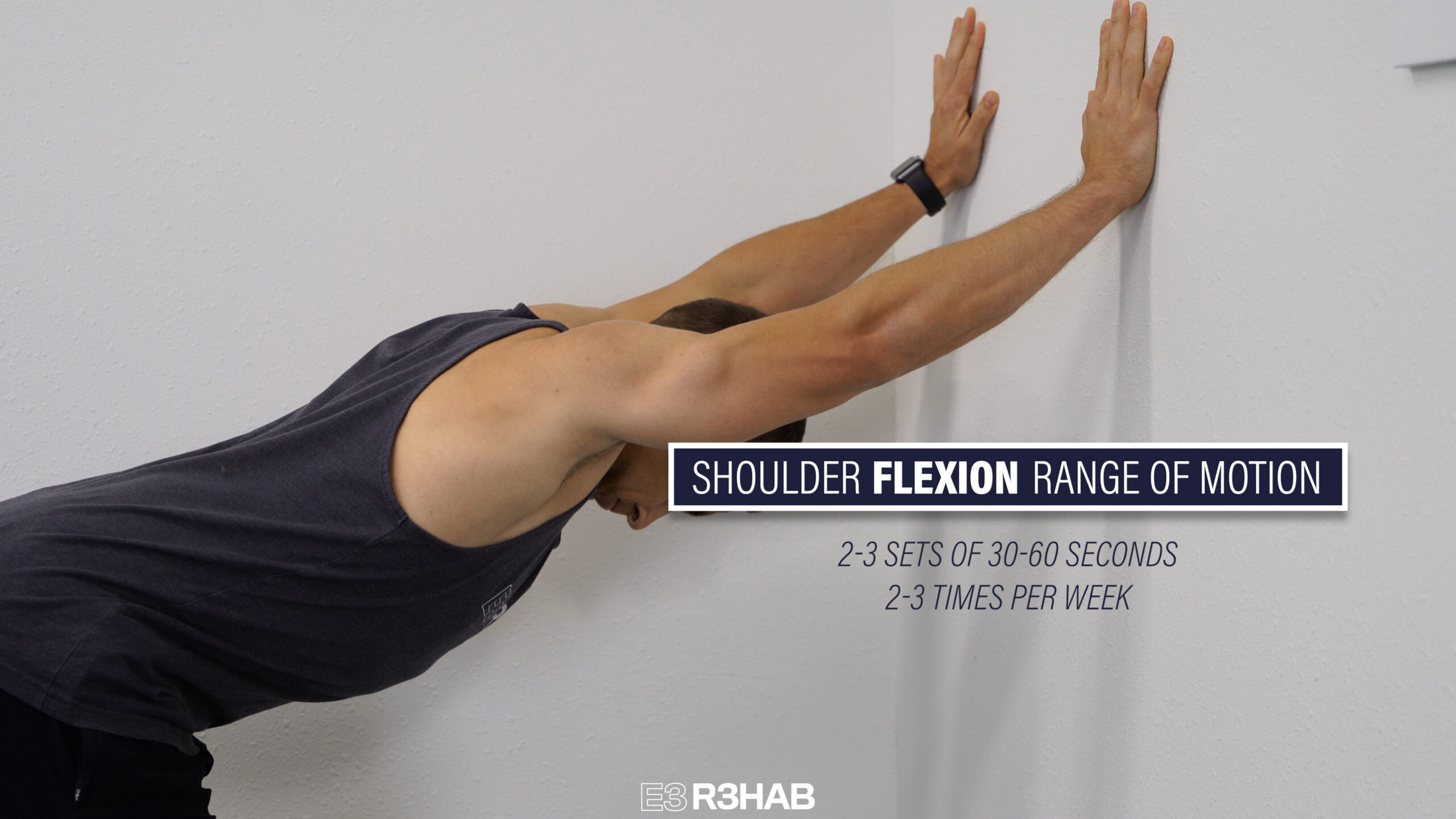
Lastly, you can work on your overhead range of motion if you notice that it’s limited or negatively affecting your day-to-day activities.
The primary option is supine shoulder flexion with a dowel. Lie on your back with your knees bent and slowly move your arms overhead as far as comfortable while holding onto a stick, PVC pipe, or broom with both hands. Use as much assistance from your uninvolved side as needed.
To increase the intensity, add a light weight to help move the shoulder further overhead.
To decrease the intensity, move through less range of motion. Another option is to gently rock in and out of shoulder flexion with your arms supported against the wall, on an elevated surface, or on the ground in child’s pose.
More advanced choices include pullover variations, such as with a dumbbell on a flat bench or across an object to allow for more thoracic extension.
The number of repetitions may vary based on the speed at which you perform a particular movement. Therefore, it might be helpful to think about accumulating 30-60 seconds total per set for 2-3 sets, 2-3 times per week.
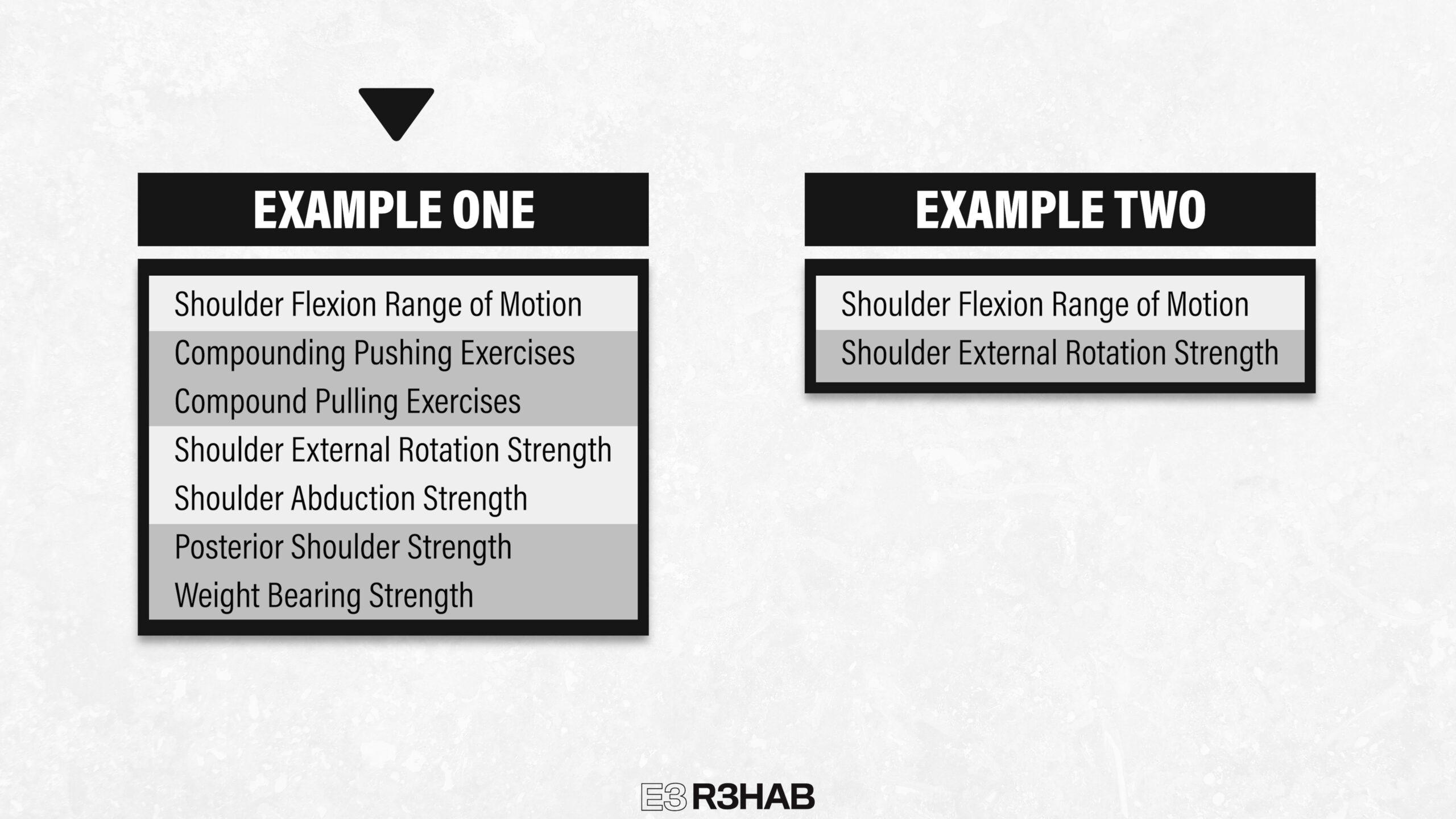
Keeping It Simple
I provided a lot of exercises, but here’s what you should know – research demonstrates that more isn’t necessarily better.Clausen 2021, Dubé 2023
For example, a study by Littlewood et al(and here) found that a single exercise is a reasonable option for improving symptoms.
What’s probably most important is that the routine you choose fits your lifestyle so you can focus on being consistent, making sure it’s tolerable, and gradually progressing over time.
If you’re an athlete or a regular gym-goer, you might try to incorporate most of what I recommended.
For someone else, you might just pick 1 or 2 categories to work on.
Do you want a structured plan that’s going to provide you with the knowledge and tools to feel more confident, capable, and resilient than ever before? Check out our Shoulder Resilience Program!
Want to learn more? Check out some of our other similar blogs: