

Do you have pain associated with your sacroiliac joint?
In this blog, I’m going to discuss sacroiliac joint pain, dispel the most common myths about the sacroiliac joint, and teach you everything you need to know about managing symptoms.
Be sure to also check out our Low Back Resilience Program!
Sacroiliac Joint Anatomy & Function
The sacroiliac joint (SIJ) refers to the connection between your sacrum, the triangle-shaped bone at the base of your spine, and your innominate (“having no name”), or pelvic bone. There are two joints, one on each side.

The joints are strongly reinforced by the surrounding ligaments and further supported by various muscles and connective tissue, such as the gluteus maximus and thoracolumbar fascia.
A primary function of the sacroiliac joint is to transfer large forces between the trunk and legs.
Sacroiliac Joint Pain
Sacroiliac joint pain may follow a traumatic event, such as a motor vehicle accident or fall onto the buttock. It can also result from repetitive activities, such as lifting or running. In some cases, the cause of symptoms is unknown. However, sacroiliac joint pain is most commonly related to pregnancy. Ostgaard 1991, Chou 2004, Gutke 2006
It is typically characterized by one sided pain below the level of the lumbar spine that may radiate into the buttock or thigh. Fortin 1994, Slipman 2000, Young 2003, Han 2023, Szadek 2023
In the physical therapy setting, a series of tests known as the Laslett Cluster are used to help rule in or rule out the diagnosis.
In the medical setting, diagnostic injections are typically used.
Unless another diagnosis is suspected, imaging is not usually warranted as findings of degeneration are normal in asymptomatic individuals and become increasingly common as we age.
I do want to highlight that some cases of sacroiliac joint pain are associated with inflammatory conditions, such as ankylosing spondylitis and psoriatic arthritis, so visiting a medical doctor may be necessary.
Sacroiliac Joint Myths
Many treatment plans for sacroiliac joint pain are based on the premise that the sacroiliac joint is fragile, unstable, and dysfunctional.
A paper by Sturesson et al found that the average movement of the sacroiliac joint is 2.5 degrees of rotation and .7mm of translation, and there are no differences between symptomatic and asymptomatic joints. This was measured using highly sophisticated technology.
There’s research going back over two decades showing that it is not possible for clinicians to feel changes in the position or movement of the sacroiliac joint. If imaging using implanted markers beneath the skin can only detect .3mm of translation or .5 degrees of rotation during frequently used tests, it is understandable that this cannot be reliably felt by the hands of clinicians or observed by the naked eye.
Even if it was possible, clinicians do not have the ability to change the position of the sacroiliac joint. For example, a paper by Tullberg et al titled “Manipulation does not alter the position of the sacroiliac joint,” found that manipulations, or adjustments, improved patients’ symptoms without causing any structural changes.
Pregnancy & Ehlers-Danlos Syndrome
What about women who are pregnant or people with Ehlers-Danlos Syndrome?
What I’m saying is not meant to invalidate their experience. There’s no denying that ligamentous laxity and sacroiliac joint movement are increased in certain individuals and during specific times. However, this is not a justification for clinicians to promote their ability to feel or change that movement with their hands, as the research indicates that neither is possible.
There’s also research demonstrating that the degree of laxity in pregnant women is not associated with their severity of pain.
Sacroiliac Joint Rehab Overview
What is the purpose of rehab then?
Well, it’s relatively simple if we consider the three mechanisms of injury that I discussed earlier:
- Physical trauma (e.g. motor vehicle accident)
- Repetitive activities (e.g. lifting or running injury)
- Spontaneous symptoms (unrelated to the inflammatory conditions that I previously mentioned)
If you’re experiencing symptoms and impairments in function after a traumatic incident, like a motor vehicle accident or fall, the goal of rehab is to get you back to your prior level of function.
If you’re struggling with a specific activity, like running or lifting, the goal of rehab is to improve your overall capacity and ability to better tolerate that activity.
If you can’t recall a distinct mechanism of injury and you have no activity-related goals, the adaptations from regular exercise may still allow you to better tolerate the demands of your day-to-day life. Plus, the benefits of exercise in general are countless and should not be overlooked.
Exercises do not need to focus on specific “stabilizing muscles.” Instead, I’m going to demonstrate a variety of exercises that train all of the muscles around the sacroiliac joints, low back, and hips. They’re appropriate for all fitness levels based on the modifications I’m going to provide.
If you feel overwhelmed by the amount of options, don’t worry, I’m going to show you how these exercises can be tailored to meet your individual needs and goals.
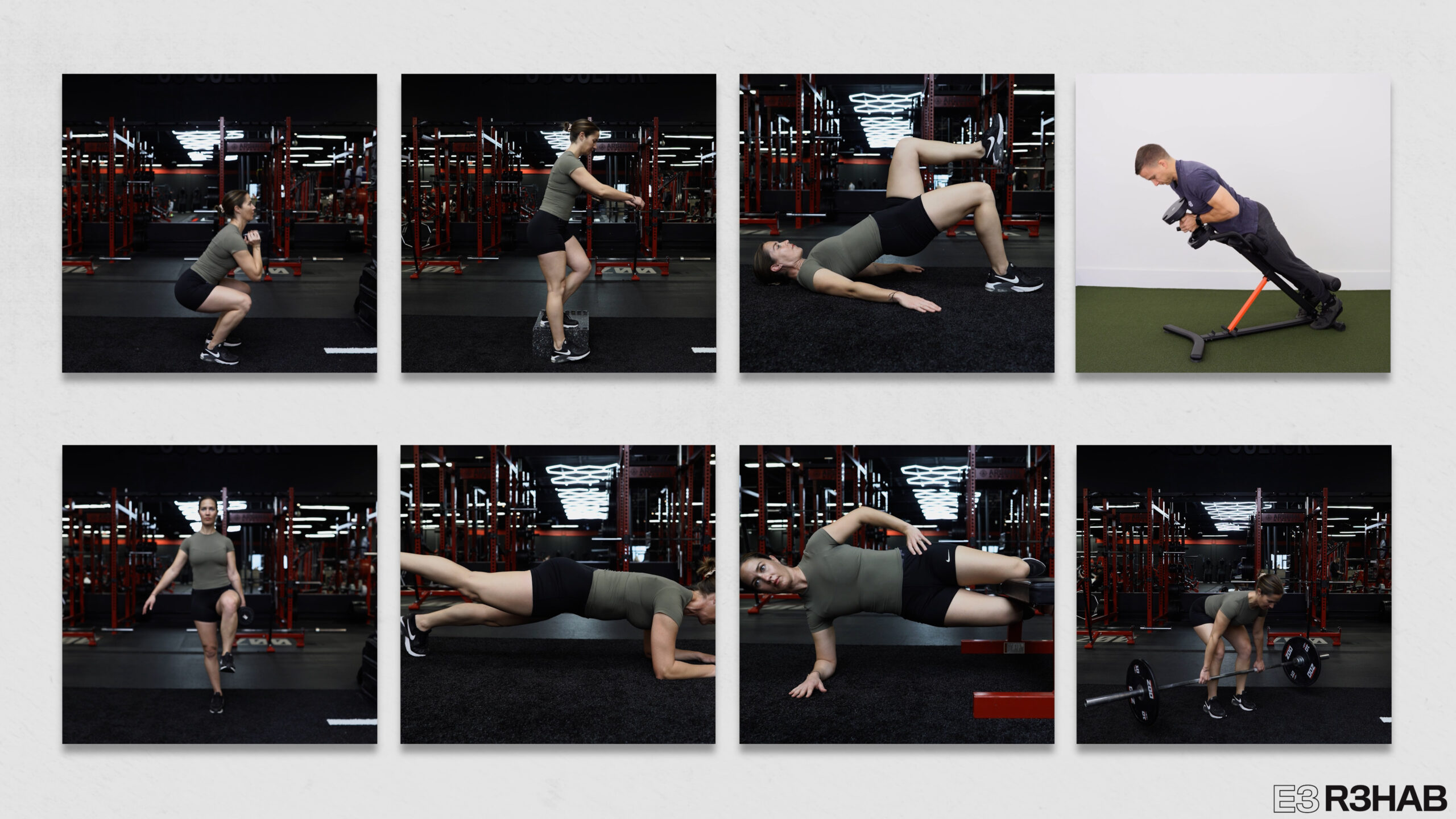
Sacroiliac Joint Exercises
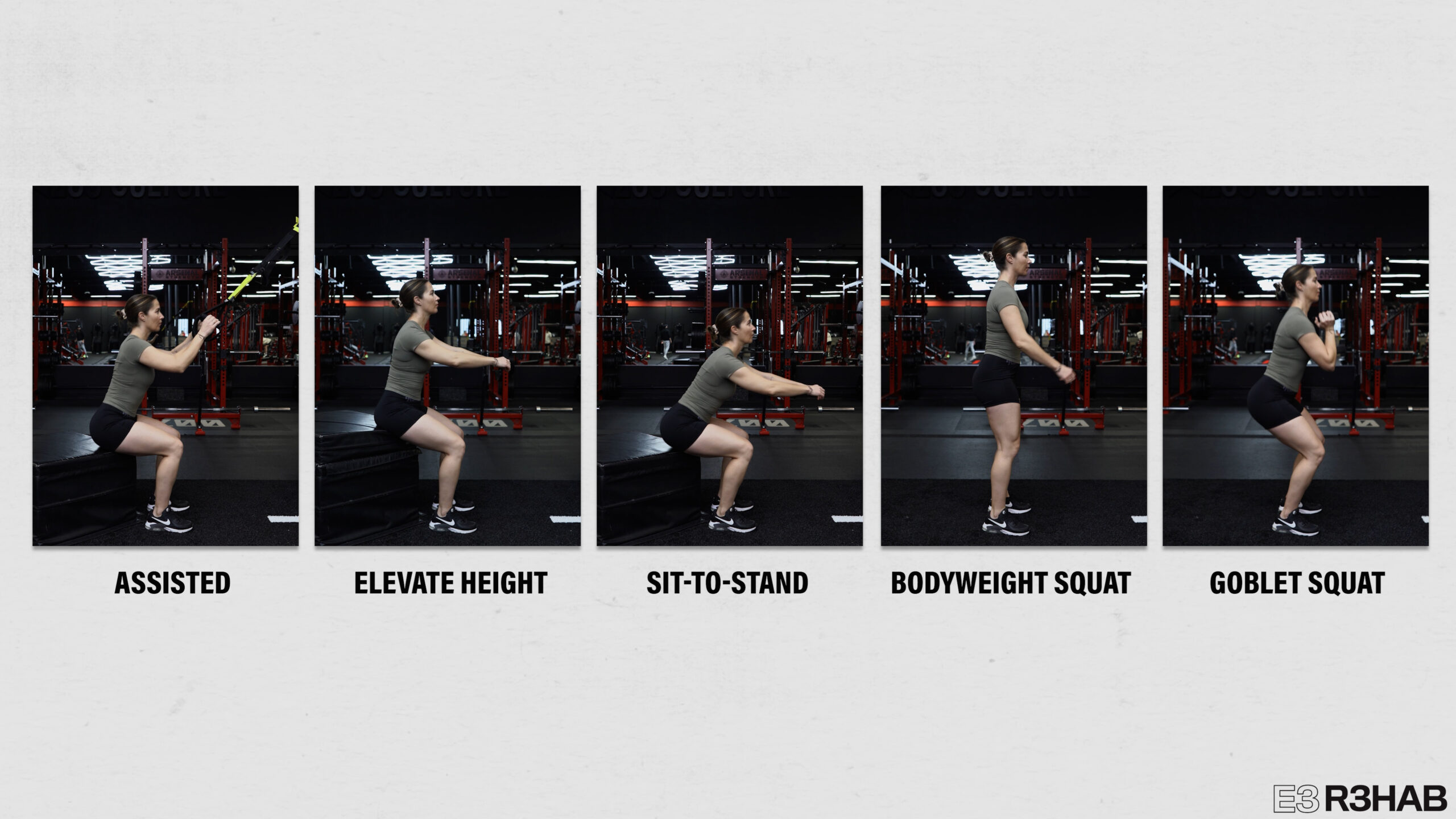
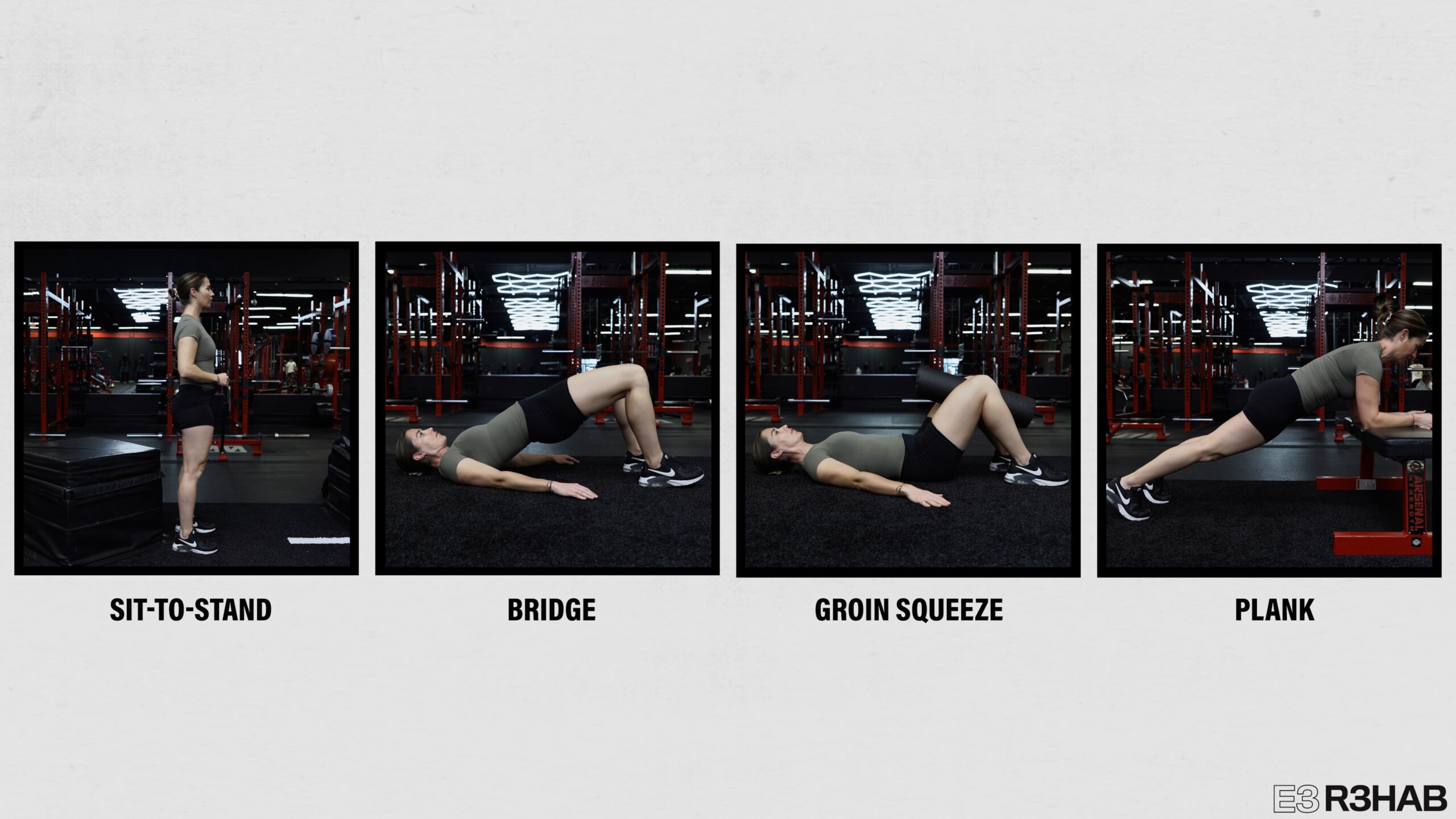
Let’s start with the basics. It’s not unusual for people to experience pain when getting up from a sitting position. Therefore, sit-to-stands from a chair are a great place to start. If you want to make them easier, you can elevate the height of the seat or use your hands for assistance. If you want to make them harder, you can do bodyweight squats. From there, you can progress to holding a weight in your hands.
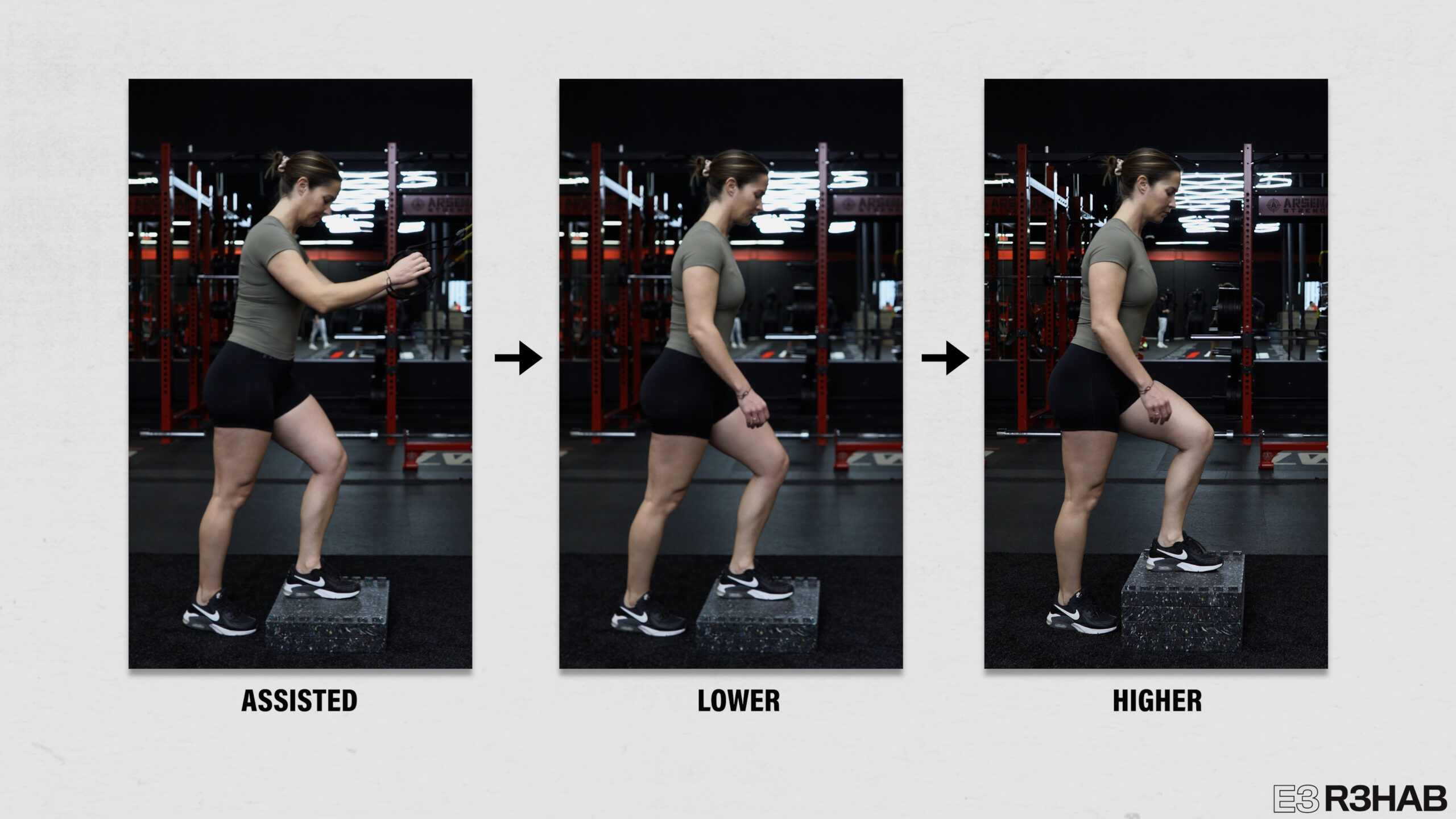
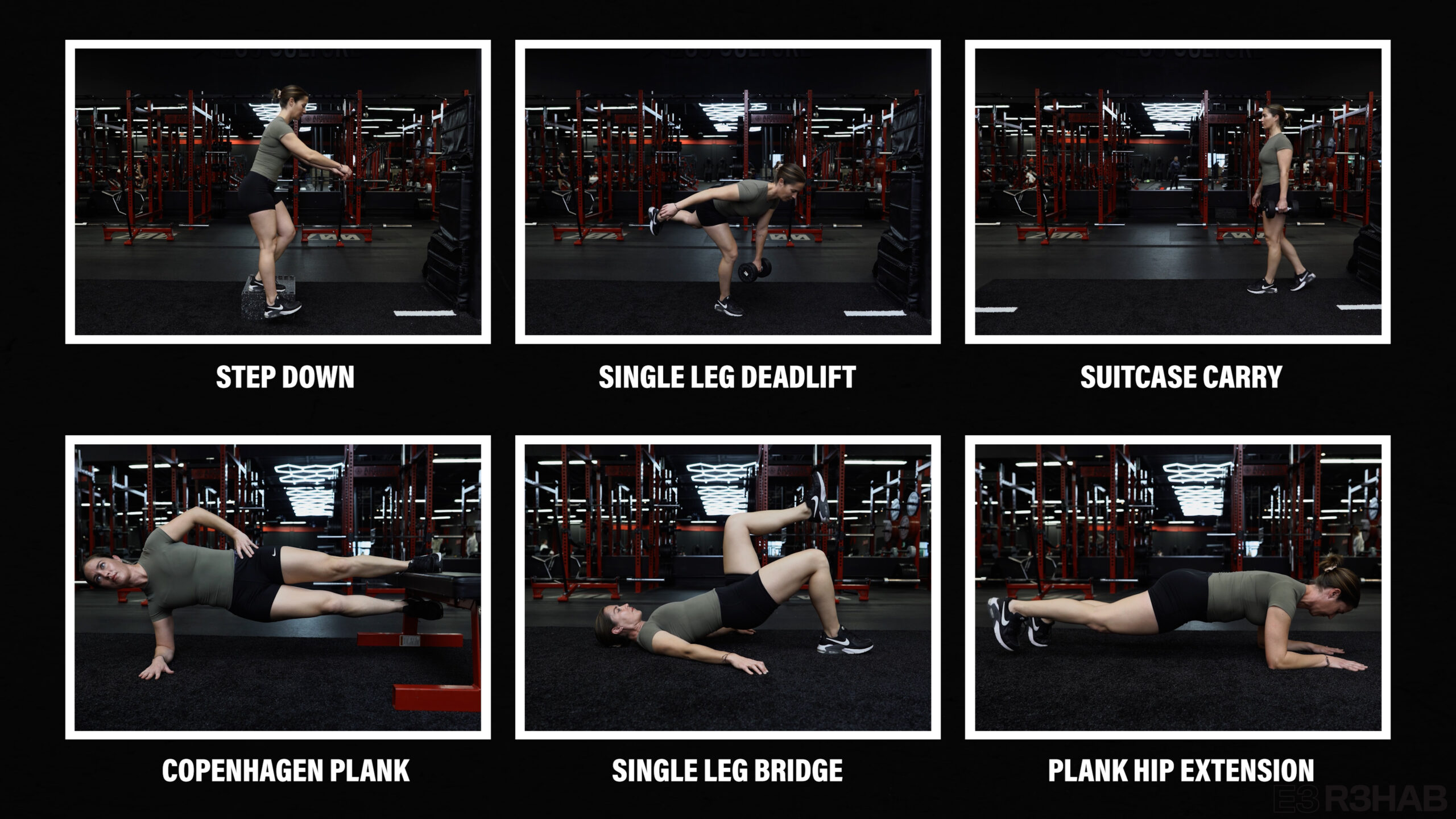
If you’re struggling with stairs or putting weight on one leg, step ups and step downs are useful.

You can use actual stairs or a small, sturdy object and progress the height over time. You can also use your hands for assistance here.
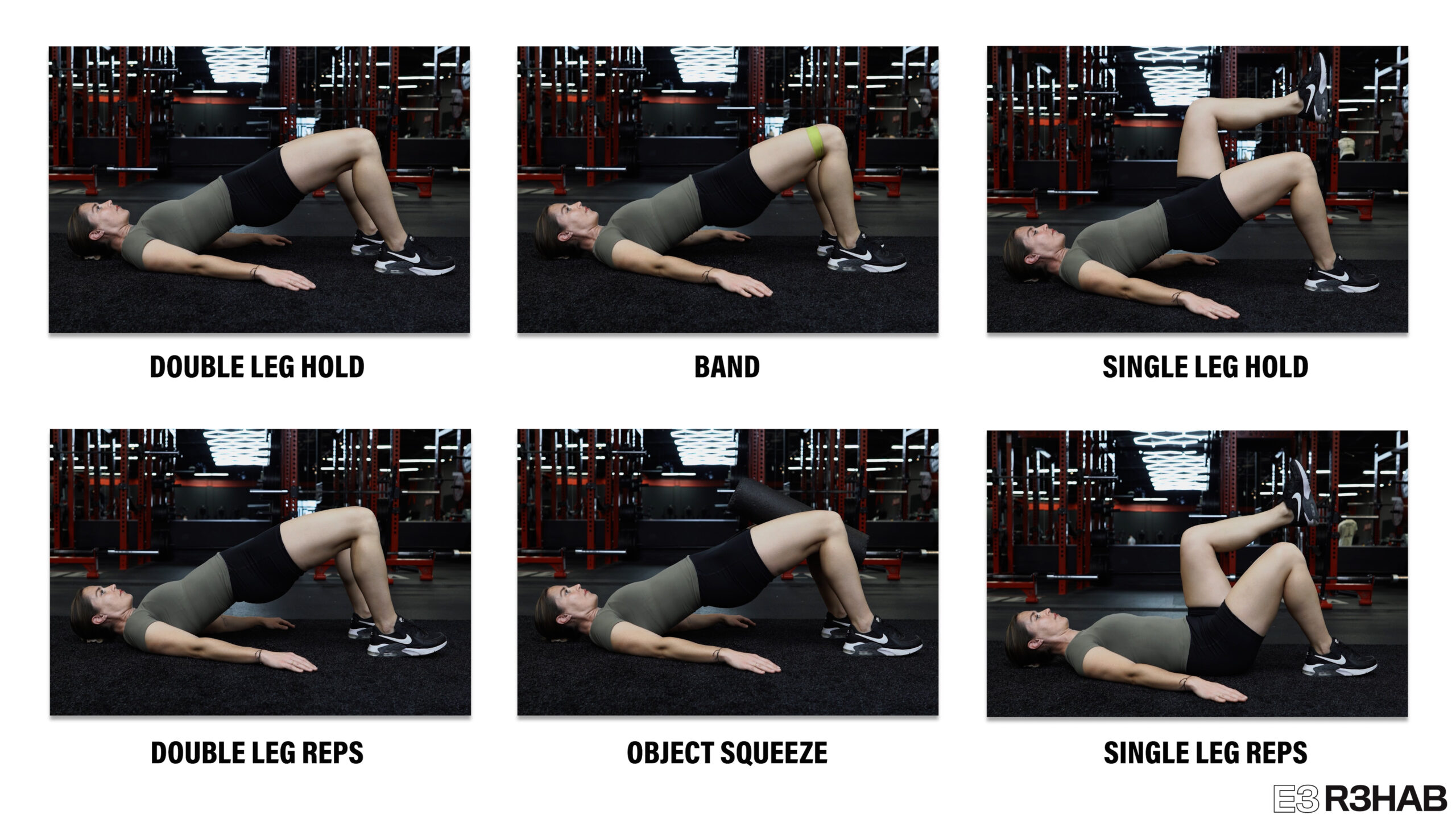
To train the glutes and low back, bridges can be used. Depending on what’s comfortable, you can either do an isometric, in which you just hold the top position, or perform actual repetitions. Some people like to add a band around the knees or squeeze an object between the knees. To make bridges harder, do the holds or repetitions one leg at a time.
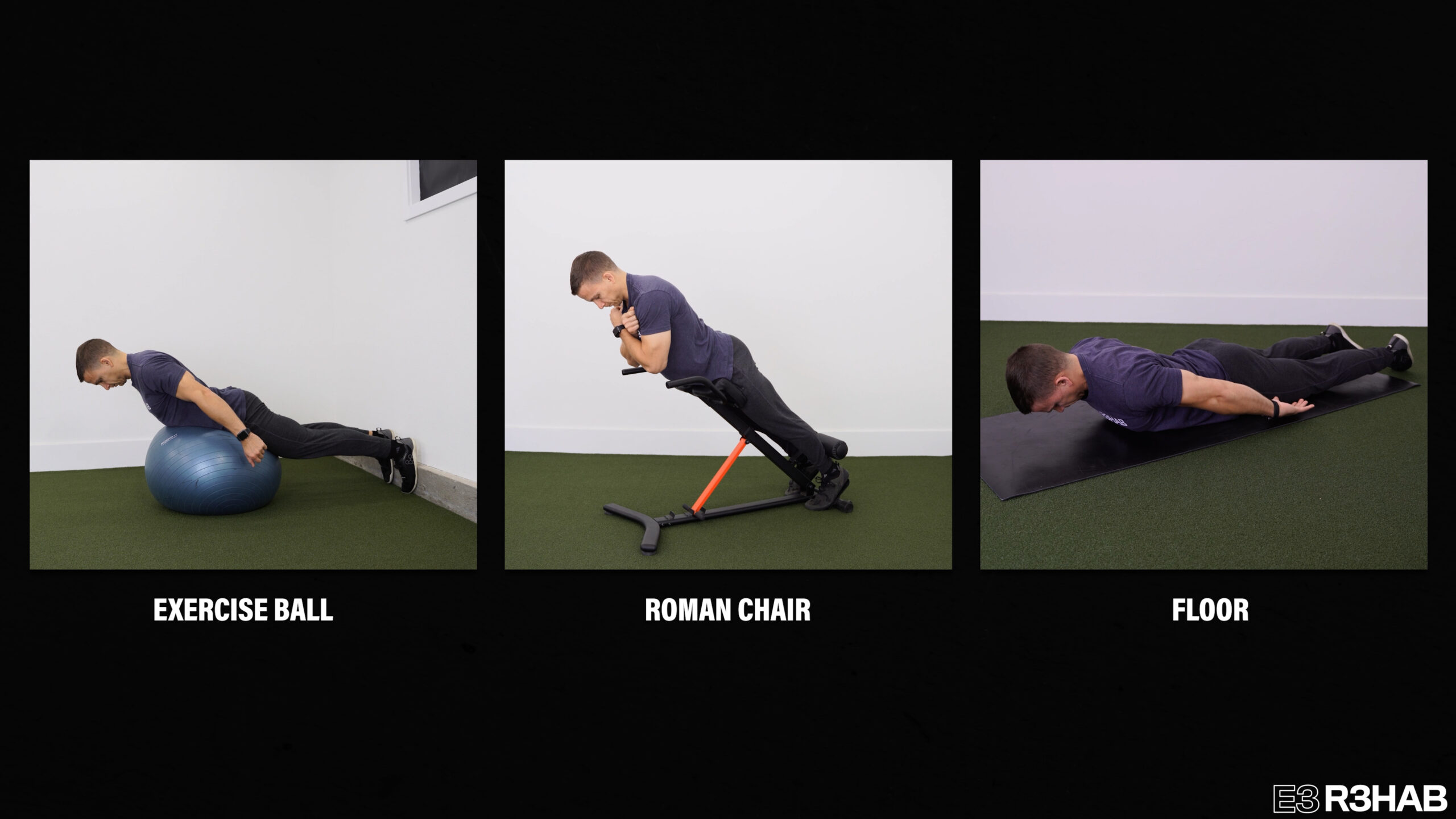
Another option for training the muscles of the low back is the back extension exercise, which can be done on an exercise ball, Roman Chair, or on the floor.
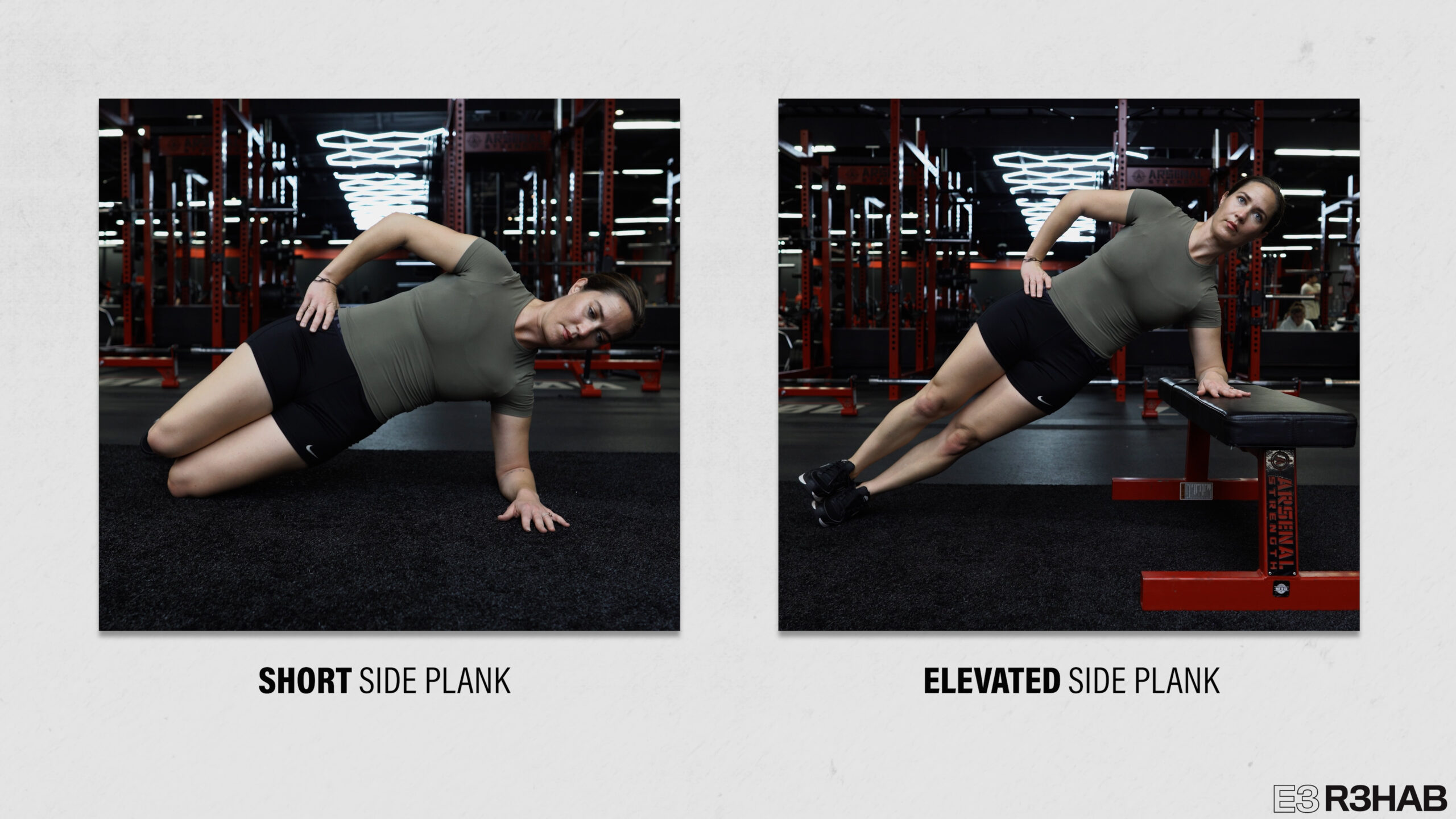
To train the sides of the trunk and hips, you can perform a side plank.

To make it easier, do a short side plank on your forearm and knees or a shoulder elevated side plank.
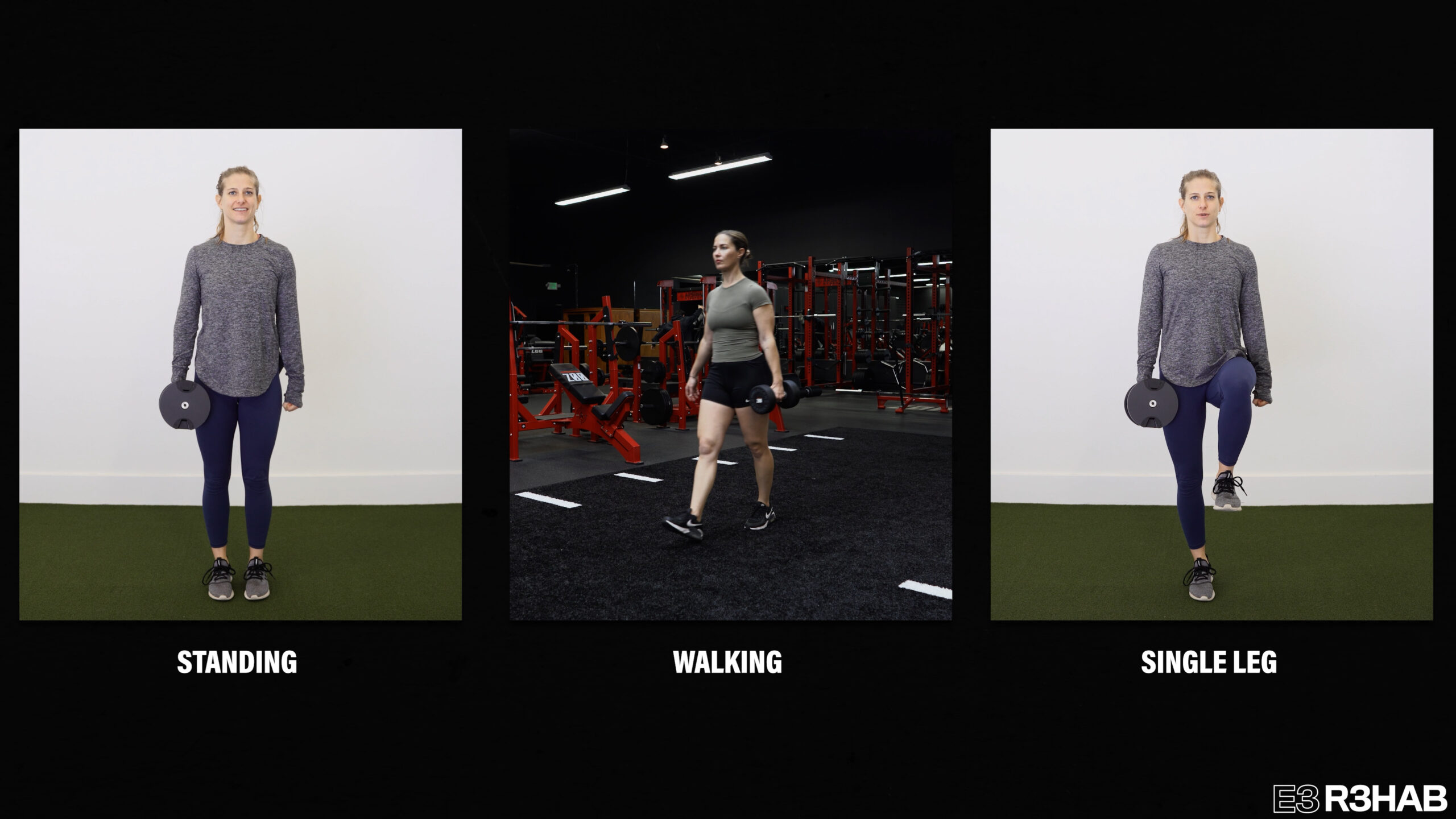
Another option for training these muscles is the suitcase carry, in which you hold a weight in one hand. You can do this while standing upright, walking, or while standing on one leg.
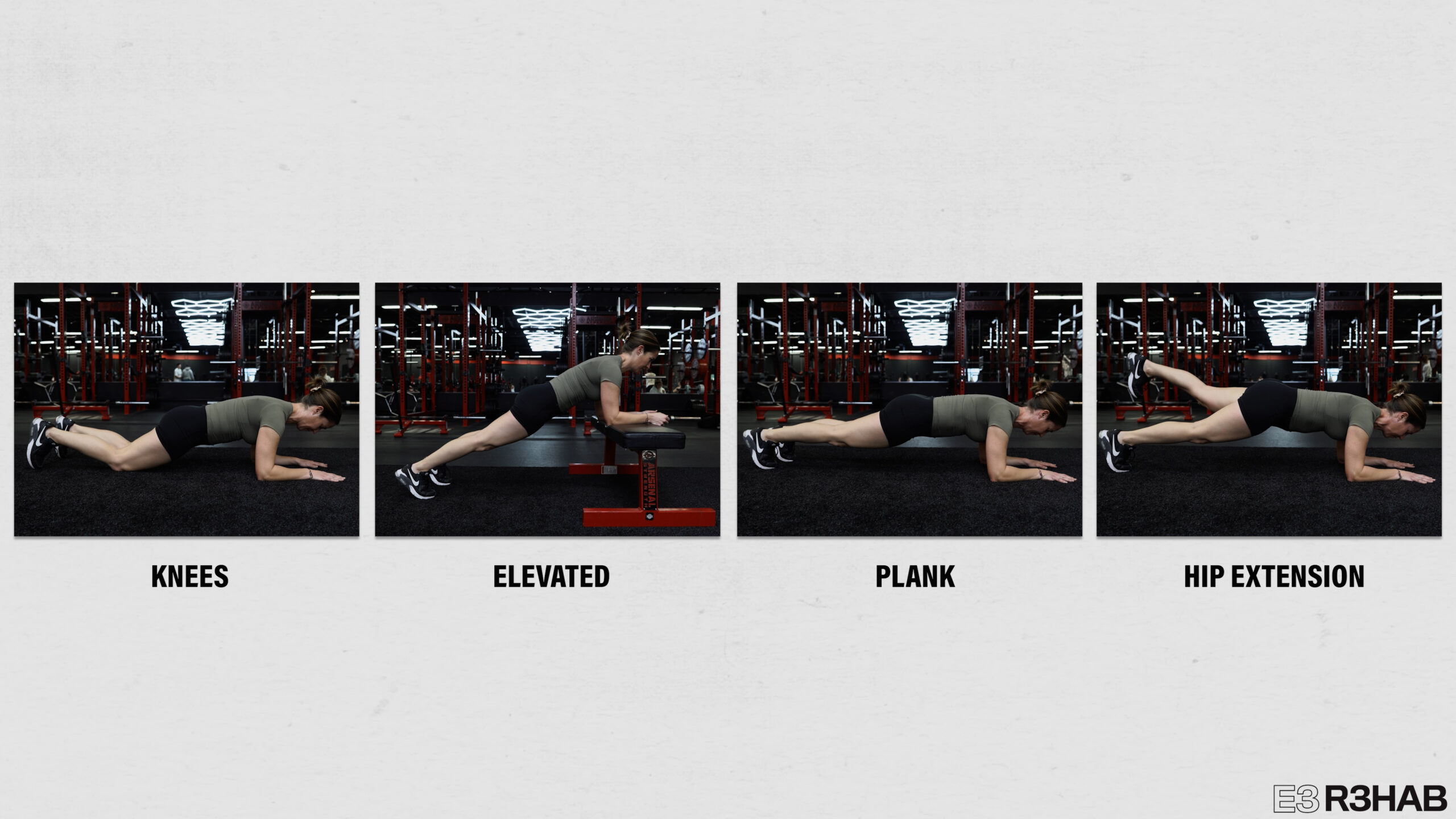
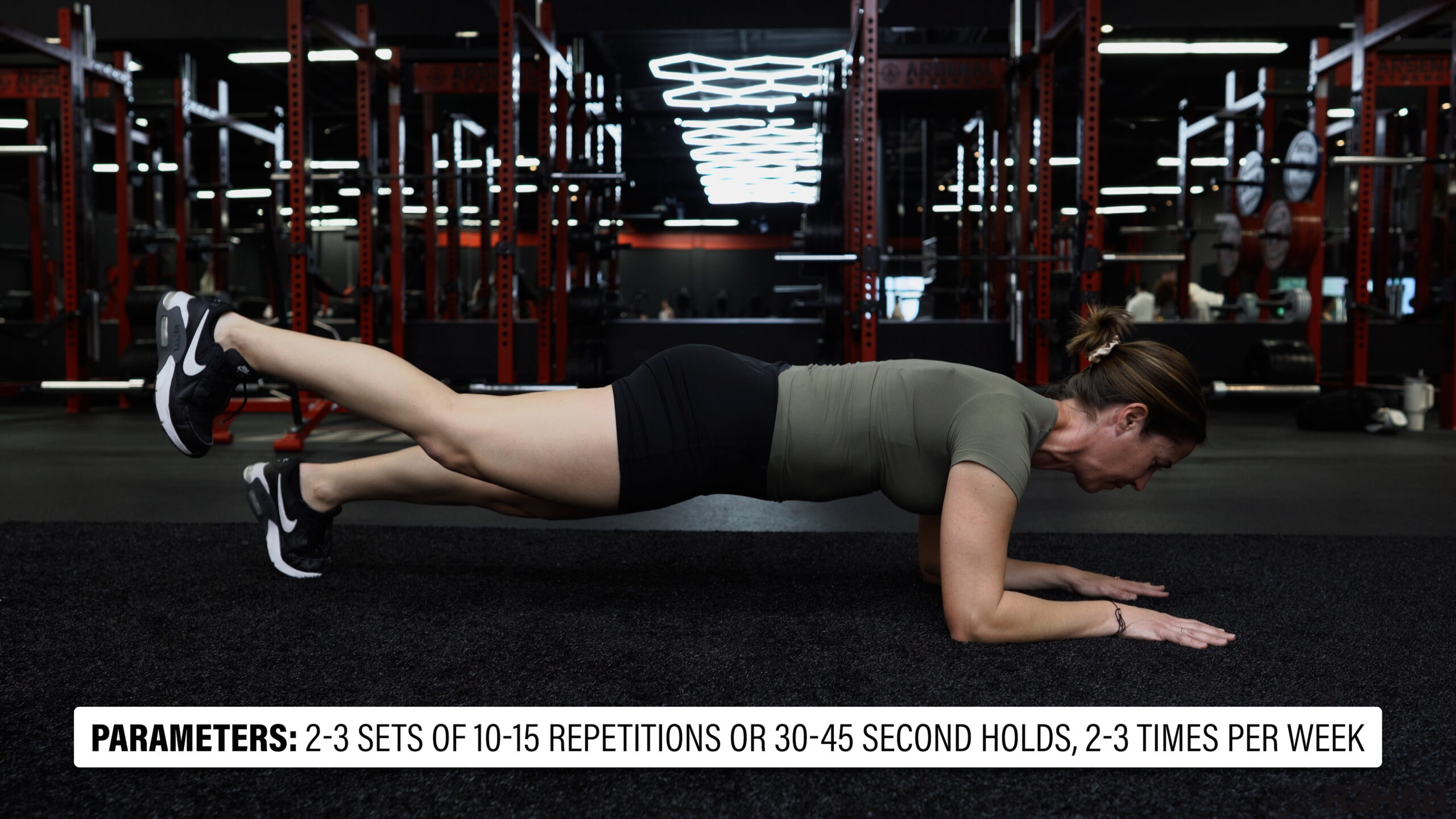
To train the front of the trunk and hips, planks can be performed. To make them easier, do them on your knees or elevate your forearms. To make them more difficult for your hips, you can perform alternating hip extension.
I already discussed how you can squeeze an object between your knees while performing bridges, but you can also do this without performing bridges to just work the groin muscles. Squeeze less or more to make it easier or harder.

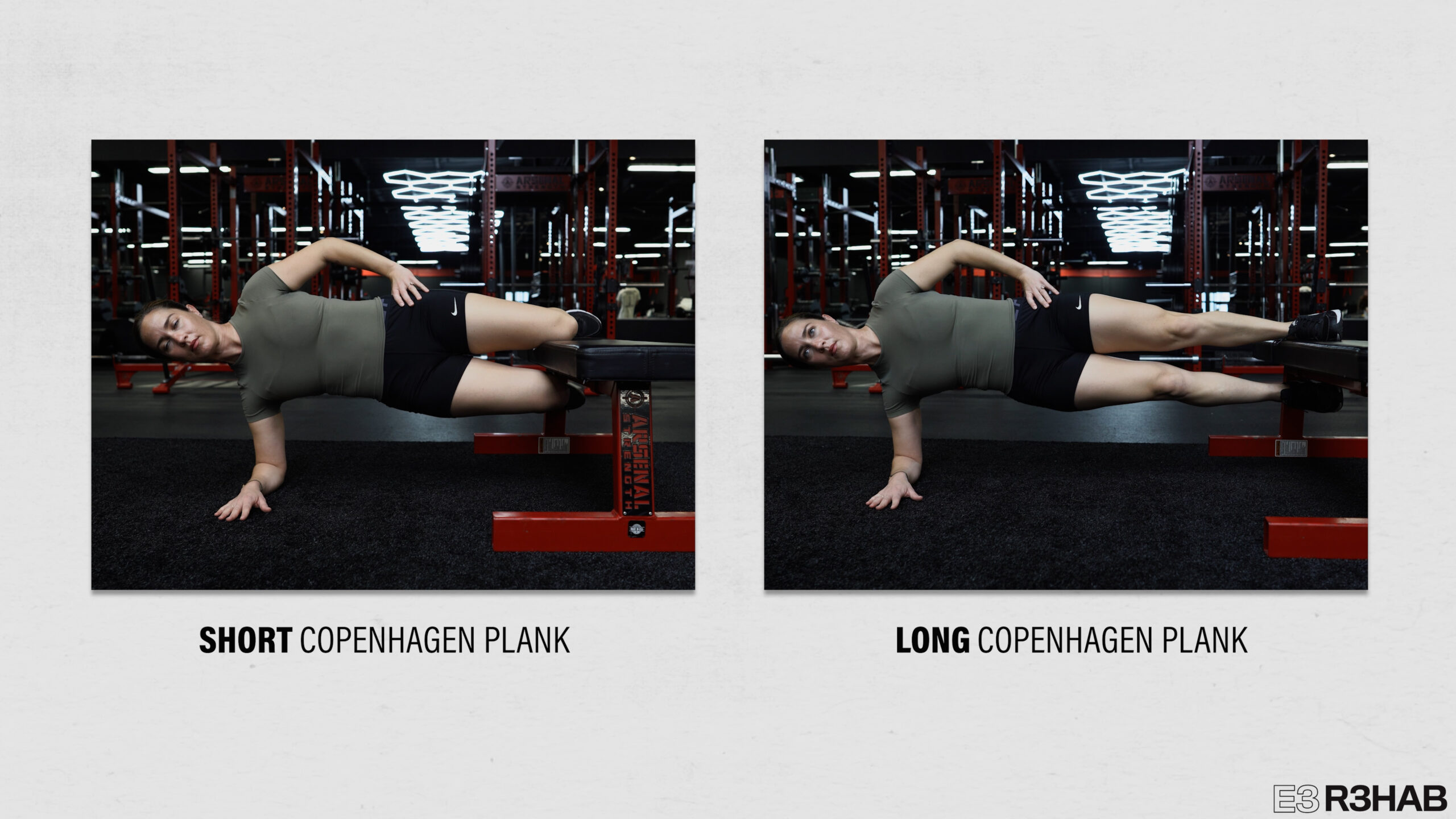
An advanced groin exercise is the Copenhagen plank with the inside of your thigh or ankle on a bench.
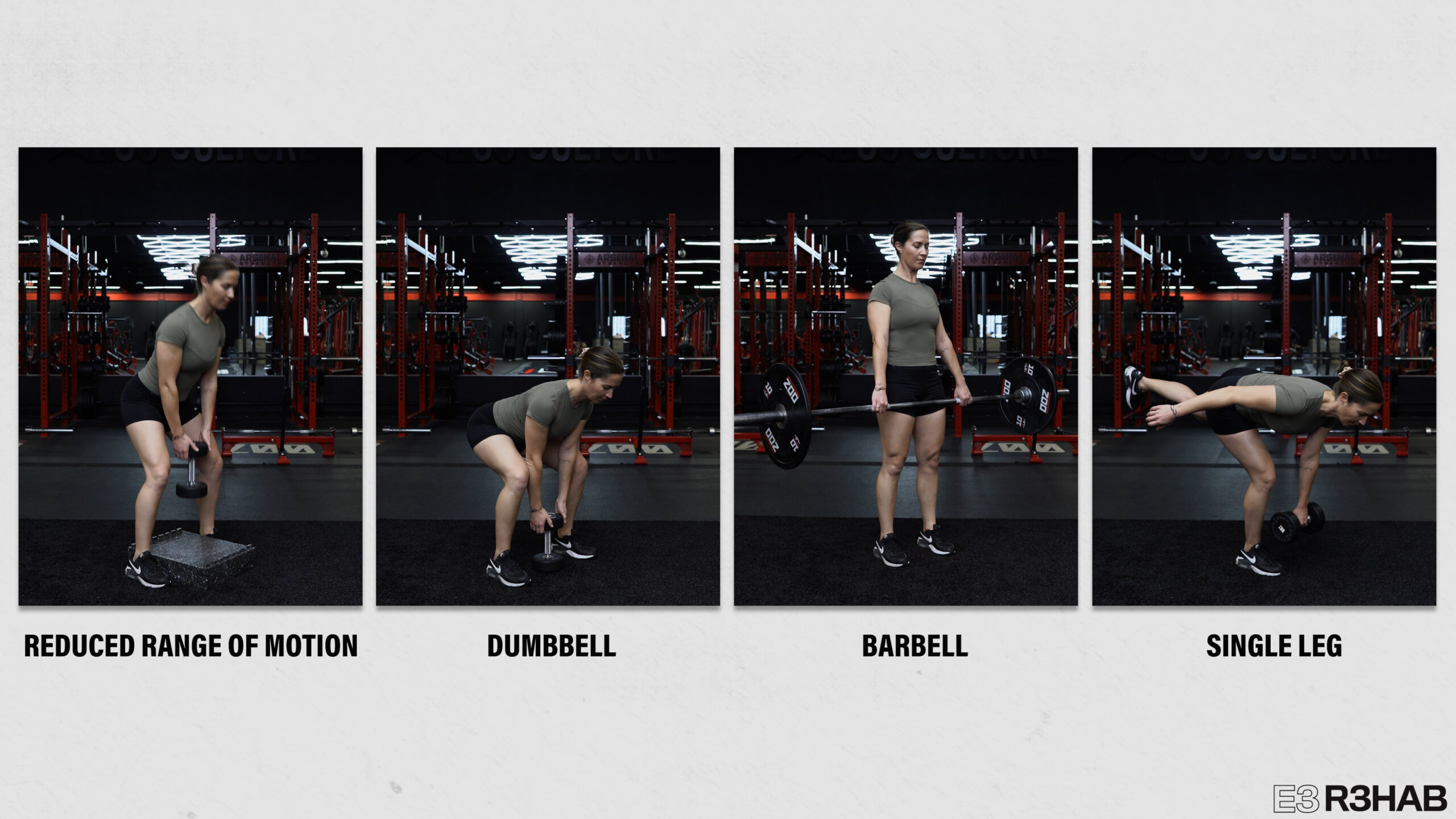
Lastly, if you’re struggling with reaching down or picking up objects from the floor, a deadlift with a kettlebell or dumbbell is a good starting point. Use a reduced range of motion if needed. Then increase the weight, use a barbell, or perform single leg deadlifts as desired.
Any of these exercises can be performed for 2-3 sets of 10-15 repetitions or 30-45 second holds, 2-3 times per week.
If you’re suffering from severe pain, you might focus on the sit-to-stands, bridges, and groin squeezes. Eventually you can add in other exercises as tolerable, such as the planks.
If you’re a runner who is pretty far along in your rehab process, you might be doing step downs, single leg deadlifts, suitcase carries, Copenhagen planks, single leg bridges, and the planks with alternating hip extension.
The point is for you to take what you need and leave what you don’t. No matter what you do, start easy and build slowly. Rehab takes time, patience, and consistency.
Sacroiliac Joint Belt, Stretches, and Self-Adjustments
What about sacroiliac joint belts, stretches, and self-adjustments?
Although they don’t change the mobility of the sacroiliac joint, there is moderate evidence to suggest that external pelvic compression can help reduce pain.
If you get relief from certain stretches you found online, there’s no harm in doing those stretches.
Similarly, if you benefit from performing self-adjustments or movements that make your sacroiliac joint pop, that’s completely fine. The pop is just a gas bubble being released, which is why there’s a delay before you can experience that pop again.
Do you want a structured plan that’s going to provide you with the knowledge and tools to feel more confident, capable, and resilient than ever before?
Check out our Low Back Resilience Program!
Want to learn more? Check out some of our other similar blogs:
Core Stability, Glute Training, Anterior Pelvic Tilt
Thanks for reading. Check out the video and please leave any questions or comments below.


