

In this blog, I’m going to tell you why your shoulder hurts and what you should do about it!
Be sure to also check out our Shoulder Resilience Program!
Basic Shoulder Anatomy
The shoulder complex is made up of 3 different joints:
- Glenohumeral Joint (what most people think of when discussing the shoulder)
- Acromioclavicular Joint
- Sternoclavicular Joint

The glenohumeral joint, often referred to as a ball-and-socket joint, is where the glenoid fossa of the scapula, or shoulder blade, meets the head of the humerus, or arm bone. The shallow socket of the shoulder allows it to be the most mobile joint in the body.
The labrum (labeled “glenoid lig” in the image below) is a fibrocartilaginous ring that increases the depth of that socket and improves the stability of the shoulder. The tendon of the long head of the biceps brachii muscle partially blends with the top portion of the labrum. I’ll revisit the importance of this relationship later.

The glenohumeral joint is then surrounded by a connective tissue known as the joint capsule.
The three rotator cuff muscles located on the back of the shoulder blade are the supraspinatus, infraspinatus, and teres minor. The rotator cuff muscle located on the front of the shoulder blade is the subscapularis.

Although these muscles contribute to individual joint actions of the shoulder, such as external rotation, internal rotation, and abduction, they are most well known for their role in providing “dynamic stability,” which means they actually help control and support the shoulder with every movement.

This is largely due to the fact that they are somewhat interconnected, surround most of the shoulder, and blend together with the joint capsule.
The acromioclavicular, or AC, joint is the connection between the acromion of the scapula and the distal end of the clavicle, or collarbone. It is supported by a joint capsule, the acromioclavicular ligament, and the coracoclavicular ligament, which consists of two parts: the trapezoid and conoid ligaments.

Ligaments attach from bone to bone and provide passive joint stability. An injury to a ligament is known as a sprain.
Lastly, the sternoclavicular joint is where the proximal end of your clavicle meets the top of your sternum.
Sternoclavicular Joint Injuries
Compared to the other diagnoses I’m going to discuss, sternoclavicular joint injuries are relatively uncommon. Traumatic injuries, resulting in sprains, dislocations, or fractures, typically follow motor vehicle accidents, collisions in contact sports, or falls. In non-traumatic cases, such as an older individual with osteoarthritis or younger person with hypermobility, symptoms may include pain, tenderness, stiffness, popping, or subluxations, especially with overhead movements.

Acromioclavicular (AC) Joint Injuries
An AC joint injury is usually the result of a direct force to the top part of the acromion, such as a fall on the shoulder with the arm at the side. It can also occur from falling on an outstretched hand (FOOSH). More severe injuries may result from a motor vehicle accident.
An AC joint injury is classified according to the Rockwood classification system via an x-ray.
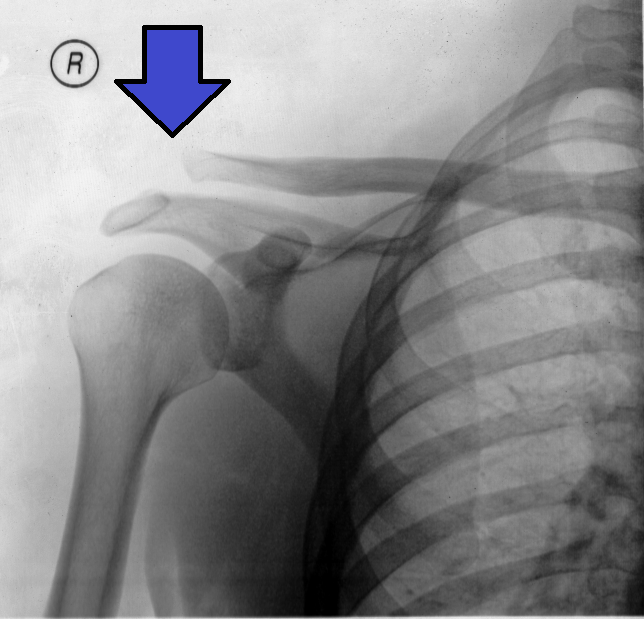
There are 6 types:
Type 1 – involves a mild sprain of only the acromioclavicular ligament.
Type 2 – consists of a ruptured acromioclavicular ligament and joint capsule, and a mild sprain of the coracoclavicular ligament.
Type 3 – both ligaments and joint capsule are ruptured and the distal end of the clavicle is moderately elevated.
This type often presents with a piano key sign, where applying downward pressure on the distal clavicle causes temporary reduction. Upon releasing the pressure, the clavicle returns to an elevated position, similar to pressing a piano key.
Type 4 – presents similarly to type 3 but with a posteriorly displaced distal clavicle, possibly penetrating the trapezius muscle.
Type 5 – the distal clavicle is severely elevated and there is a high probability that both the deltoid and trapezius muscles are detached from the clavicle.
Type 6 – the distal end of the clavicle is inferiorly displaced under the coracoid process of the scapula (behind the coracobrachialis and short head of the biceps tendon).

Symptoms can include swelling, limitations in range of motion, and pain with lying on the affected shoulder.

Additionally, pain may be felt toward the top or front of the shoulder when moving the arm across the body (horizontal adduction), overhead, and behind the back (extension) since these place more stress on the AC joint.

In severe cases (types 3-6), a visible deformity may occur due to the displacement of the distal clavicle.
Since this injury results from trauma, it is important to rule out other diagnoses, such as a clavicle fracture, injury to the sternoclavicular joint, and any neurovascular involvement.
In the event of an AC joint injury, there are two primary treatment options: nonoperative management and surgery.
For a low-grade type 1 or type 2 injury, nonoperative management should be the first line of treatment in most cases.
For more severe injuries (types 3-6), various factors, such as a person’s symptoms, function, goals, and response to rehabilitation, will influence the decision to have surgery or not.
It is also worth noting that since more severe injuries (types 3-6) have a displaced clavicle, the cosmetic appearance of the shoulder may play a role in someone’s decision to have surgery.

Want to learn more?
Check out our full blog about Acromioclavicular Joint Injury Rehab!
Glenohumeral Joint Diagnoses
When it comes to the shoulder, pain can often be divided into 3 broad categories:
- The Stiff Shoulder, like Frozen Shoulder or Adhesive Capsulitis
- The Unstable Shoulder, which relates to a history of dislocations or subluxations
- The Weak & Painful Shoulder

Under this umbrella of the weak and painful shoulder are the following diagnoses (among others):
- Rotator Cuff Tears
- Shoulder Impingement
- Rotator Cuff Tendinitis or Tendinopathy
- Biceps Tendinopathy
- Subacromial Pain Syndrome
- Rotator Cuff Related Shoulder Pain

Frozen Shoulder
Frozen shoulder, frequently referred to as adhesive capsulitis, is a clinical diagnosis most commonly seen in women between the ages of 40 and 65. Individuals usually present with a gradual onset of pain and stiffness that’s often worse at night and negatively impacts sleep.

There are two types of frozen shoulder.
For people with primary frozen shoulder, also called idiopathic frozen shoulder, the exact cause is unknown.
On the other hand, secondary frozen shoulder is associated with diabetes, thyroid disorders, stroke, trauma, and various shoulder pathologies.

Individuals with frozen shoulder will present with passive external rotation loss that is greater than 50% of their uninvolved shoulder, or less than 30°.

Deficits in range of motion of greater than 25% in 2 other planes are also expected.
For example, shoulder flexion and abduction may be limited by 25% or more compared to the other shoulder.

X rays are not necessary, but can help rule in or out other conditions, such as severe osteoarthritis.
Frozen shoulder is sometimes characterized by 3 overlapping stages:
- A “freezing” phase, in which pain worsens.
- A “frozen” phase, in which stiffness peaks.
- A “thawing” phase, in which symptoms gradually improve.

This is a simplified framework though as symptoms may take up to 2 years or longer to resolve. Rehabilitation, as well as lifestyle modifications to diet and exercise habits when appropriate, are recommended to regain full function.

Unfortunately, there are no quick fixes. For this reason, aggressive, painful stretching is NOT recommended.
Want to learn more?
Check out our full blog about Frozen Shoulder Rehab!
Shoulder Dislocations & Instability
Moving on to shoulder instability, there are 2 main types.
The first is traumatic which results in a partial or complete separation of the glenohumeral surfaces, commonly known as a subluxation or dislocation. This is usually the result of falling on an outstretched hand or from a direct blow to the shoulder.

About 97% of dislocations occur anteriorly, meaning the head of the humerus is forced out of the joint socket in the forward direction. They can also occur posteriorly or inferiorly, but these are rare.
Traumatic injuries typically involve structural damage, most often in the form of a Bankart lesion, which is when the anterior and inferior portions of the labrum separate from the glenoid fossa.
Other associated injuries can include:
- A Hill-Sachs lesion, which is a compression fracture of the humeral head
- A glenoid rim fracture, also known as a bony Bankart
- A neurological injury, such as damage to the Axillary nerve
- A rotator cuff tear
Before reducing a dislocation, or putting it back into its normal position, X-rays are performed to determine the direction and if there are any other injuries, like a fracture.
The second type of instability is atraumatic, which may happen without any history of a significant preceding injury. An example would be a swimmer who developed pathological laxity from repetitive overuse. There may be structural abnormalities found in the shoulder, but they are not a result of a single traumatic experience.
It is also worth noting that the presentation of shoulder instability can change over time. For instance, someone who had a traumatic anterior shoulder dislocation may develop recurrent instability years later.
Other classification systems include a third type that is also atraumatic, but is defined by a loss of muscle control without structural damage. These are less common, but someone with Ehlers-Danlos Syndrome would fall into this category.

It’s important to understand that shoulder laxity or hyperlaxity by itself is just a sign, while shoulder instability is a term associated with clinical symptoms.
These symptoms can include pain, apprehension, and feelings of instability with various movements or positions, such as when your arm is away from your body or when reaching back behind you.

Regardless if you have traumatic or atraumatic instability, management options include surgery and rehabilitation, or rehabilitation alone.
For anterior shoulder dislocations, multiple studies show that younger athletes who received stabilization surgery experienced lower rates of recurrent instability and decreased need for future surgery compared to those who received nonoperative management only. Handoll et al 2004, Belk et al 2021, Alkhatib et al 2022, Zaremski et al 2016
For atraumatic instability, a 2023 randomized, placebo-controlled trial found that surgery, where the joint capsule was “tightened”, did not lead to better results than a placebo surgery in terms of improvement in pain and functional impairments.
These studies provide some insight, but the decision to undergo surgery is nuanced, as it depends on various factors such as age, sport, type of instability, degree of tissue damage, etc.
In the cases of atraumatic instability, rehabilitation is often the first-line recommendation. However, in some cases, if symptoms do not improve, referral to an orthopedic surgeon might be necessary.
Want to learn more?
Check out our full blog about Shoulder Dislocation & Instability Rehab!
SLAP Tears
Symptomatic SLAP tears can involve deep shoulder pain, as well as popping, clicking, or catching.
SLAP stands for “Superior Labrum, Anterior and Posterior.” In other words, the top of the labrum, front and back.
Snyder and colleagues, who introduced the term in 1990, described 4 types of SLAP tears:
- Type 1 involves fraying or degeneration of the superior labrum. The labrum remains attached with the biceps tendon intact.
- Type 2 is characterized by detachment of the superior labrum and biceps tendon.
- Type 3 is a bucket-handle tear of the superior labrum with the biceps tendon intact.
- Type 4 is a bucket-handle tear of the superior labrum that extends into the biceps tendon.
Although additional types and subtypes have been presented, the original classification by Snyder continues to be the most recognized and referenced in research and practice.
When SLAP tears result from acute trauma, they are often categorized as compression-type injuries or traction-type injuries. The most common compression-type injury involves falling on an outstretched hand (FOOSH). Traction-type injuries involve a sudden pull, such as when water skiing, grabbing something overhead to stop a fall, or losing hold of a heavy object.
Traumatic injuries can also involve motor vehicle accidents or a direct blow to the shoulder.
On the other hand, chronic injuries are typically attributed to throwing in sport or other repetitive overhead activities.
However, not all SLAP tears need to be categorized as injuries because “abnormalities” of the labrum found on imaging are actually quite common in asymptomatic individuals.
For example, a study by Schwartzberg et al in 2016 investigated 53 adults between the ages of 45 and 60 and discovered superior labral tears in 55% to 72% of these participants despite them having no symptoms. A study by Lansdown et al in 2018 suggests that SLAP tears become increasingly prevalent with aging.
Tears of the labrum are also common in athletes, especially those involved in overhead sports, such as volleyball and baseball. Miniaci 2002, Lesniak 2013, Del Grande 2016, Pennock 2018, Hacken 2019
For instance, a study by Cooper et al in 2022 examined asymptomatic, elite-level rock climbers and reported that “Labral pathology was present in 69% of shoulders, with discrete labral tears identified in 56%.”
Therefore, nonoperative management is often the first-line recommendation.
Want to learn more?
Check out our full blog about SLAP Tear Rehab!
The Weak & Painful Shoulder
Let’s move on to the diagnoses that fall under the umbrella of “the weak and painful shoulder,” including rotator cuff tears, bursitis, and shoulder impingement.
It’s often believed that imaging, injections, and surgery are required for these conditions, but in general, exercise therapy is the first-line recommendation because symptoms related to any of these diagnoses likely have more to do with current tissue sensitivity from sudden or gradual changes in activity and your overall health as opposed to compression of structures, excessive local inflammation, or new tears of your rotator cuff.
Rotator Cuff Tears
A systematic review by Teunis et al stated the following: “The prevalence of rotator cuff abnormalities in asymptomatic people is high enough for degeneration of the rotator cuff to be considered a common aspect of normal human aging and to make it difficult to determine when an abnormality is new (e.g., after a dislocation) or is the cause of symptoms.”
Am I talking about partial-thickness tears or full-thickness tears?
Both.
A recent study by Hinsley et al found that 48.4% of full-thickness tears were asymptomatic in the population studied.
How is this possible?
Rotator cuff tears are often thought to be like a rope cut in half, but they’re more similar to a hole in a piece of cloth due to their interconnecting nature that I discussed at the beginning.

The cloth still works fine, which is why many people don’t experience pain or changes in function despite having a rotator cuff tear.
Does that mean surgery is never indicated? No. You should always consult with your medical doctor before making any decisions, especially if trauma was involved.
However, exercise is safe and recommended because shoulder activity level is not related to tear progression risks, tears don’t always progress in size, and an increase in tear size doesn’t necessarily mean a worsening of function or symptoms anyway.

As I mentioned, symptoms are more about the shoulder being currently sensitive to certain positions, movements, and exercises rather than the occurrence of irreparable damage. It’s actually acceptable to have some discomfort during rehab if it’s tolerable for you and you’re slowly progressing toward your goals over time. You’re not hurting yourself.
Want to learn more?
Check out our full blog about Rotator Cuff Tear Rehab!
Shoulder Impingement
This is true for shoulder impingement, sometimes called subacromial pain syndrome, as well.
The area between the humeral head and the acromion, coracoacromial ligament, and acromioclavicular joint is known as the subacromial (under the acromion) space. Within this space is the supraspinatus tendon, long head of the biceps brachii tendon, subacromial bursa (fluid-filled sac that reduces friction), and the capsule of the shoulder joint.
When most people discuss shoulder impingement, they are referring to these tissues being compressed in this space.
The shoulder impingement theory was popularized by a surgeon in the 1970’s before he proposed a surgery to treat the issue. Since then, here’s what we’ve learned:
- If symptoms were solely caused by compression of these overlying structures, we’d expect their removal to improve symptoms and function. However, research demonstrates that subacromial decompression is no better than placebo surgery.
- Subacromial decompression also doesn’t seem to change the long-term prevalence of rotator cuff tears. As I mentioned, rotator cuff tears are present in asymptomatic individuals and are more common as we age, like many other imaging findings.
- Compression of tissues in the subacromial space is common, occurs equally in people with and without symptoms, and happens with normal, day-to-day tasks.
- A smaller subacromial space is not correlated with symptoms or disability.
So shoulder impingement exists, but it’s not the bogeyman it’s been made out to be.
This is important to know because sometimes a diagnosis can be unhelpful or even harmful, especially when up-to-date information is not provided. For example, a study found that people labeled with impingement expressed “feelings of psychological distress, uncertainty, and that the condition is serious and has a poor prognosis.” Without appropriate context, a diagnosis can negatively influence expectations, cause people to become fearful of certain movements, exercises, or activities, and act as a barrier to rehab.
This doesn’t mean that the general rehab process needs to be significantly different from what’s already being used – it’s the explanation that changes and matters:
- Exercise is safe and encouraged.
- You’re not damaging your rotator cuff when you lift your arm and experience pain.
- You don’t have to worry about removing a piece of bone to get better.
- Compression of tissues is normal in the shoulder and elsewhere. We compress nerves, tendons, ligaments, and muscles all day long when we sit, bend, lift, twist, and walk.
Want to learn more?
Check out our full blog about Shoulder Impingement!
Biceps & Rotator Cuff Tendinopathy
Tendons attach muscles to bones. When a muscle contracts, its associated tendon is affected. Despite popular belief, tendinitis is not the recommended diagnostic label for tendon-related pain because acute inflammation does not seem to be the primary driver of symptoms.

This indicates that rehabilitation does not need to focus on a predominantly anti-inflammatory approach involving ice, medication, and complete rest for an extended period of time.

“Tendinopathy” is the preferred term, which just means that there is persistent pain and loss of function associated with loading of the affected tendon. Much of the time tendinopathies are described as repetitive overuse or relative overload injuries, along the lines of “doing too much, too soon.”

Pain in the front of the shoulder is often attributed to the long head of the biceps tendon based on its location, whereas pain toward the side may be attributed to the rotator cuff.
Biceps and rotator cuff tendinopathy can occur independently or, very commonly, co-exist.
Both are related to a loss of function and pain with loading of these tendons, which can include daily tasks like reaching out, behind, or above you, or recreational activities like lifting weights and playing sports.
Want to learn more?
Check out our full blog about Biceps Tendinopathy Rehab!
What About Other Diagnoses?
What about other diagnoses and why is this information potentially so much different from what you’ve heard elsewhere?
Unfortunately, I can’t cover every possible diagnosis without making this blog longer than it already is.
Accurately diagnosing frozen shoulder, osteoarthritis, instability, and trauma-related injuries is important because these diagnoses may respond well to specific medical management, such as an early injection for frozen shoulder or surgery for an anterior shoulder dislocation. In the case of frozen shoulder, it’s also important to know that symptoms can take up to 2 years or longer to resolve.
For diagnoses like rotator cuff tendinopathy, partial rotator cuff tears, shoulder impingement, subacromial pain syndrome, rotator cuff related shoulder pain, etc., it’s often difficult to determine the exact tissue structure that may be contributing to symptoms for 2 main reasons:
- The orthopedic special tests that we use aren’t actually that special. They mostly just tell us that your shoulder hurts.
- So-called “abnormalities” on imaging are common in people who don’t have symptoms.
Uncertainty is unsettling, which is probably why many of these labels exist and why new ones get created.
However, a specific diagnosis or imaging finding doesn’t always dictate management or rehabilitation, especially for many cases that fall in the category of the “weak and painful” shoulder or symptoms that come on gradually without trauma.
What’s often more useful for me as a physical therapist is knowing your age, occupation, lifestyle, exercise habits, goals, what makes your symptoms better, what makes your symptoms worse, etc.

You might have the exact same diagnosis as someone else, but your answers to these questions could be vastly different. And those answers influence rehab.

Although rehab itself can be challenging, the goal is pretty simple – it’s to temporarily modify any aggravating activities, improve your overall health with lifestyle modifications and exercise where possible, and incorporate an exercise routine that’s manageable, tolerable, and addresses any of your deficits in strength, range of motion, confidence, etc.
Cervical Radiculopathy & Referred Pain
The last topic I want to briefly discuss is shoulder pain NOT related to the shoulder. For example, symptoms in the upper traps or the area between the shoulder blades are often caused by irritation of a nerve or other structure in the neck. If symptoms are more related to positions and movements of the neck instead of the shoulder, the neck should be suspected as the probable issue.
A less common reason for shoulder pain, although significantly more important to identify, is pain originating from the heart, lungs, gallbladder, etc. For instance, symptoms of a heart attack can include shoulder and arm pain, as well as chest and jaw pain, shortness of breath, sweating, nausea, dizziness, and more. Always consult with a medical doctor regarding any concerns.
Before wrapping up, I want to remind you that we have full-length blogs dedicated to most of these diagnoses, so please check those out if you’re looking for more in-depth information.
Do you want a structured plan that’s going to provide you with the knowledge and tools to feel more confident, capable, and resilient than ever before? Check out our Shoulder Resilience Program!

Thanks for reading. Check out the video and please leave any questions or comments below.


