

In this blog, I explain why you should stop trying to fix anterior pelvic tilt.
Looking for rehab or performance programs? Check out our store here!
What Is Anterior Pelvic Tilt?
To better understand the research and arguments I’m going to present that challenge the long-held beliefs about anterior pelvic tilt, it’s important for me to define it and briefly describe the relevant anatomy.
On the front of your pelvis, you have two bony landmarks known as the Anterior Superior Iliac Spine, or ASIS for short.

Similarly, on the back of your pelvis, you have two bony landmarks known as the Posterior Superior Iliac Spine, or PSIS.

Pelvic tilt is often portrayed as the angle created by an imaginary line drawn from the PSIS to the ASIS.

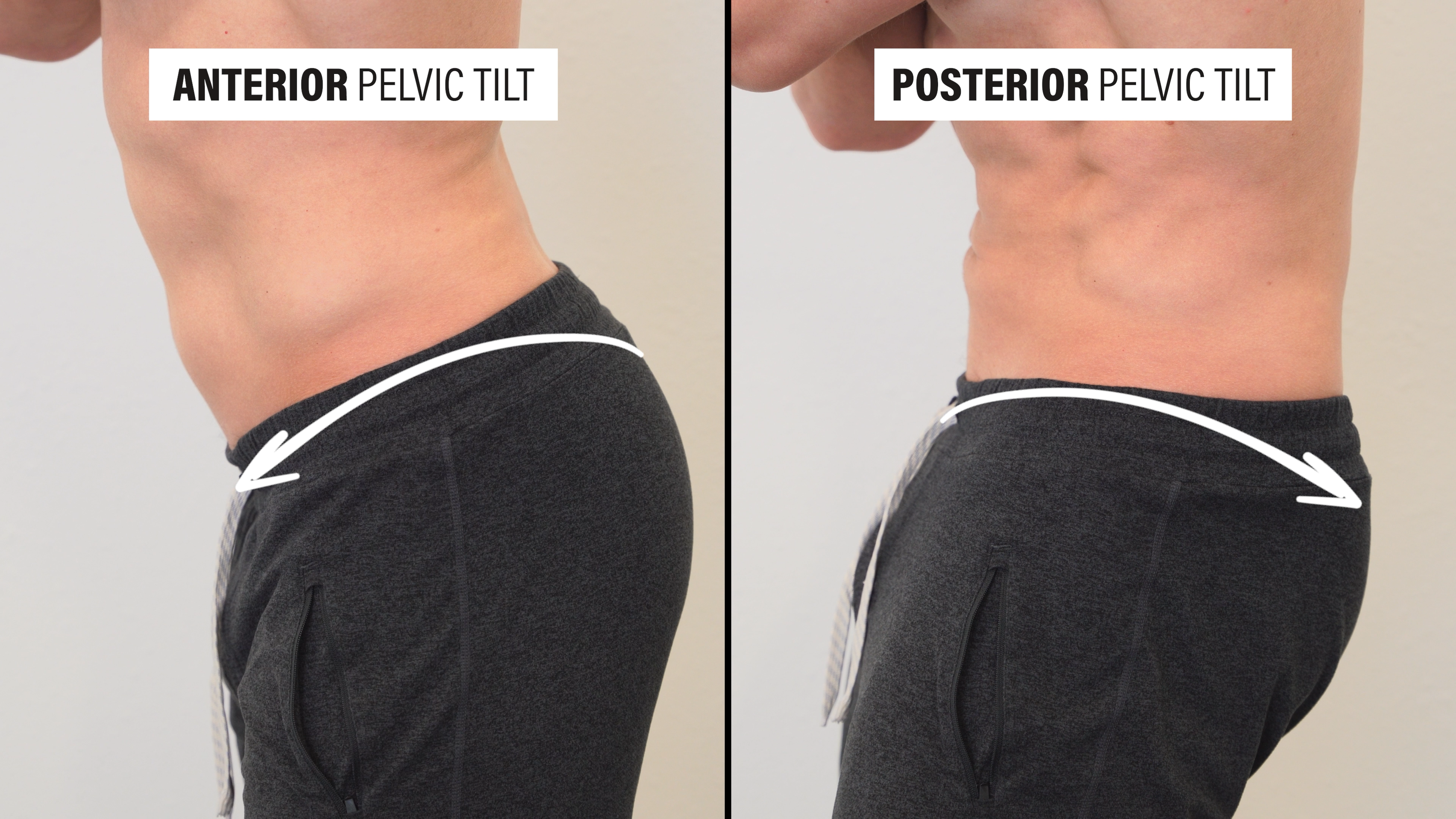
Therefore, when assessing static standing posture, 3 positions are usually described:
- Posterior Pelvic Tilt, in which the line is sloped down toward the PSIS.
- Neutral Pelvic Tilt, in which the line drawn is straight across.
- Anterior Pelvic Tilt, in which the line is sloped down toward the ASIS and our pelvis is tipped forward.
Anterior pelvic tilt is the typical standing position for most people and is associated with our normal lumbar lordosis, or arched position of the low back.

Pelvic tilt can also be described as a movement. When you actively perform an anterior pelvic tilt, your hips become more flexed while your low back becomes more extended. Alternatively, when you actively perform a posterior pelvic tilt, your hips become more extended while your low back becomes more flexed.
Picture yourself lying on your back with your hips and knees bent and feet flat on the floor. If you were to create space between your back and the floor, you’d be performing an anterior pelvic tilt.

If you were to flatten your back to the floor, you’d be performing a posterior pelvic tilt.

Why is Anterior Pelvic Tilt Supposedly Problematic?
The most commonly cited reason I see and hear about on social media or otherwise is Lower Crossed Syndrome, which was a theory proposed by a medical doctor and researcher, Vladimir Janda, in 1979.
According to Janda, anterior pelvic tilt is a result of muscle imbalances: the abs and glutes are weak, while the hip flexors and low back extensors are tight.
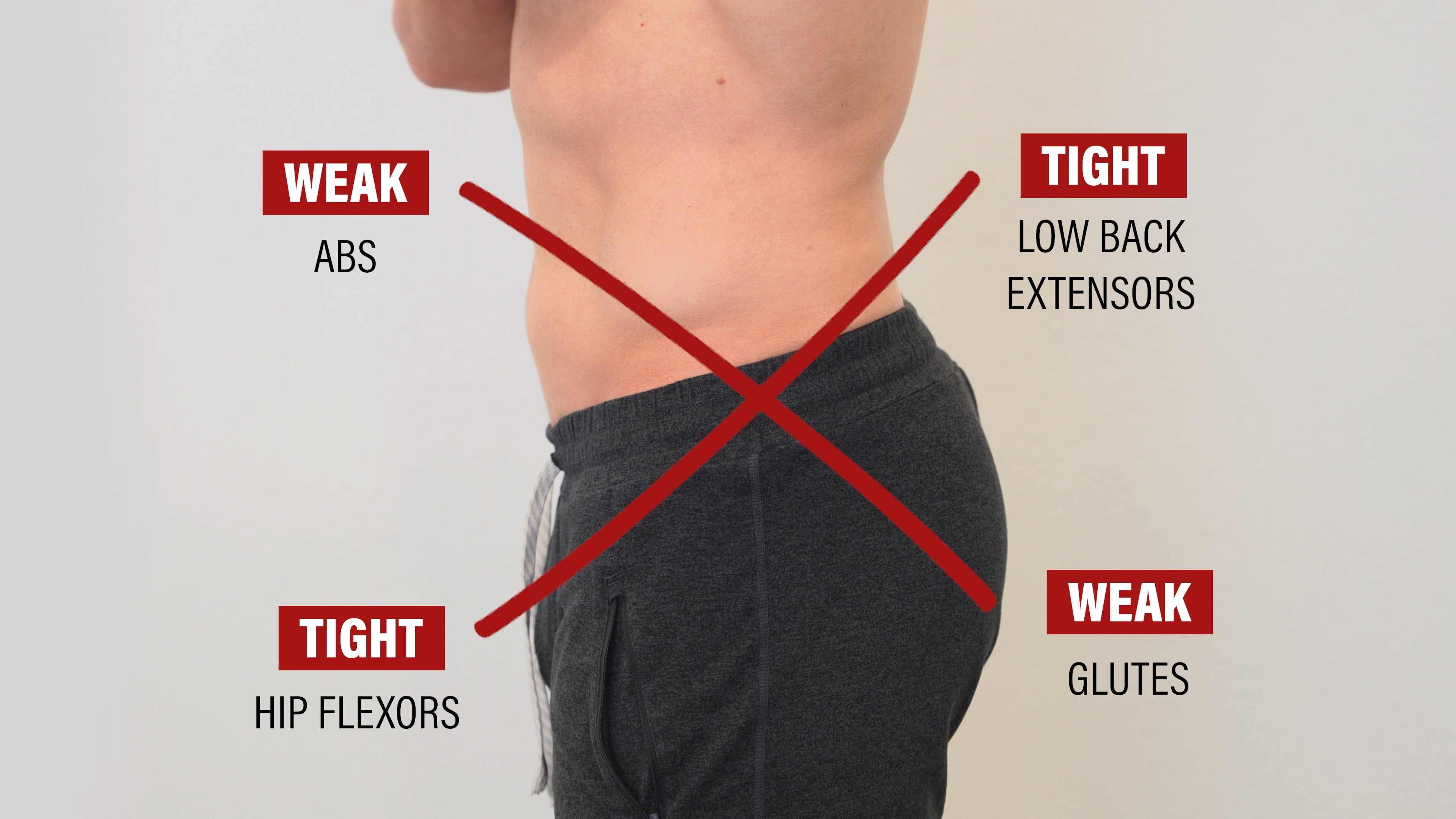
As a consequence of these muscle imbalances, low back pain, movement dysfunction, and other issues may arise.
However, as stated on the website used to preserve his teachings: “While Vladimir Janda was the first to recognize Upper Crossed Syndrome (UCS) and Lower Crossed Syndrome (LCS), few studies have validated the specific pattern of muscle imbalance and postural abnormalities associated with these common muscle imbalance syndromes.”
Since over 40 years of research has been conducted since 1979, let me share 5 reasons why you don’t need to fix anterior pelvic tilt.
You Don’t Need To Fix Anterior Pelvic Tilt
- Anterior pelvic tilt is normal.
- A study by Herrington in 2011 found that “85% of males and 75% of females presented with an anterior pelvic tilt.”
- Anterior pelvic tilt is NOT associated with low back pain.
- A systematic review by Laird et al in 2014 demonstrated that “Compared to people without low back pain, on average, people with low back pain display no difference in lordosis angle…” and “no difference in standing pelvic tilt angle…”
- In fact, a systematic review by Chun et al in 2017 reported that “Overall, patients with low back pain tended to have smaller lumbar lordotic angles than healthy controls.”
- A study by Franklin and Conner-Kerr in 1998 concluded the following: “This study suggests that from the first to the third trimester of pregnancy lumbar lordosis, posterior head position, lumbar angle, and pelvic tilt increases; however, the magnitudes and the changes of these posture variables are not related to back pain.”
- None of this is new information. A study by Dieck et al published in 1985 followed women for 25 years to determine the association between postural changes and neck and back pain. They found that women with an “…increased degree of kyphosis, lordosis, or pelvic tilt were not at an increased risk of subsequent spinal pain.”
- Anterior pelvic tilt is NOT associated with weak abs.
- Walker et al in 1987 “…found no correlation between abdominal muscle function, pelvic tilt, and lumbar lordosis.” They go on to state: “Patients often are taught abdominal muscle “strengthening” exercises as a means of altering their standing posture. The theoretical basis on which this practice has been built is not supported by our data. No apparent relationship exists between abdominal muscle function and standing pelvic tilt, abdominal muscle function and lumbar lordosis, and lumbar lordosis and pelvic tilt.”
- Youdas et al in 2000 concluded that “In patients with chronic low back pain, the magnitude of the lumbar lordosis and pelvic inclination in standing is not associated with the force production of the abdominal muscles.”
- Anterior pelvic tilt is NOT associated with weak glutes as reported by
- Anterior pelvic tilt is NOT associated with tight hip flexors, statically or dynamically, as evidenced by Heino et al in 1990 and Schache et al in 2000. On top of that, a study by Koumantakis et al in 2021 discovered that the number of sitting hours per day was not related to lumbopelvic posture. This makes intuitive sense. Despite having my elbows bent most of the day while working at the computer, using my phone, eating, and even sleeping on my side with my hands by my face, my elbows don’t get stuck in this position because I straighten them occasionally – just like you do with your hips when you stand up and walk around.
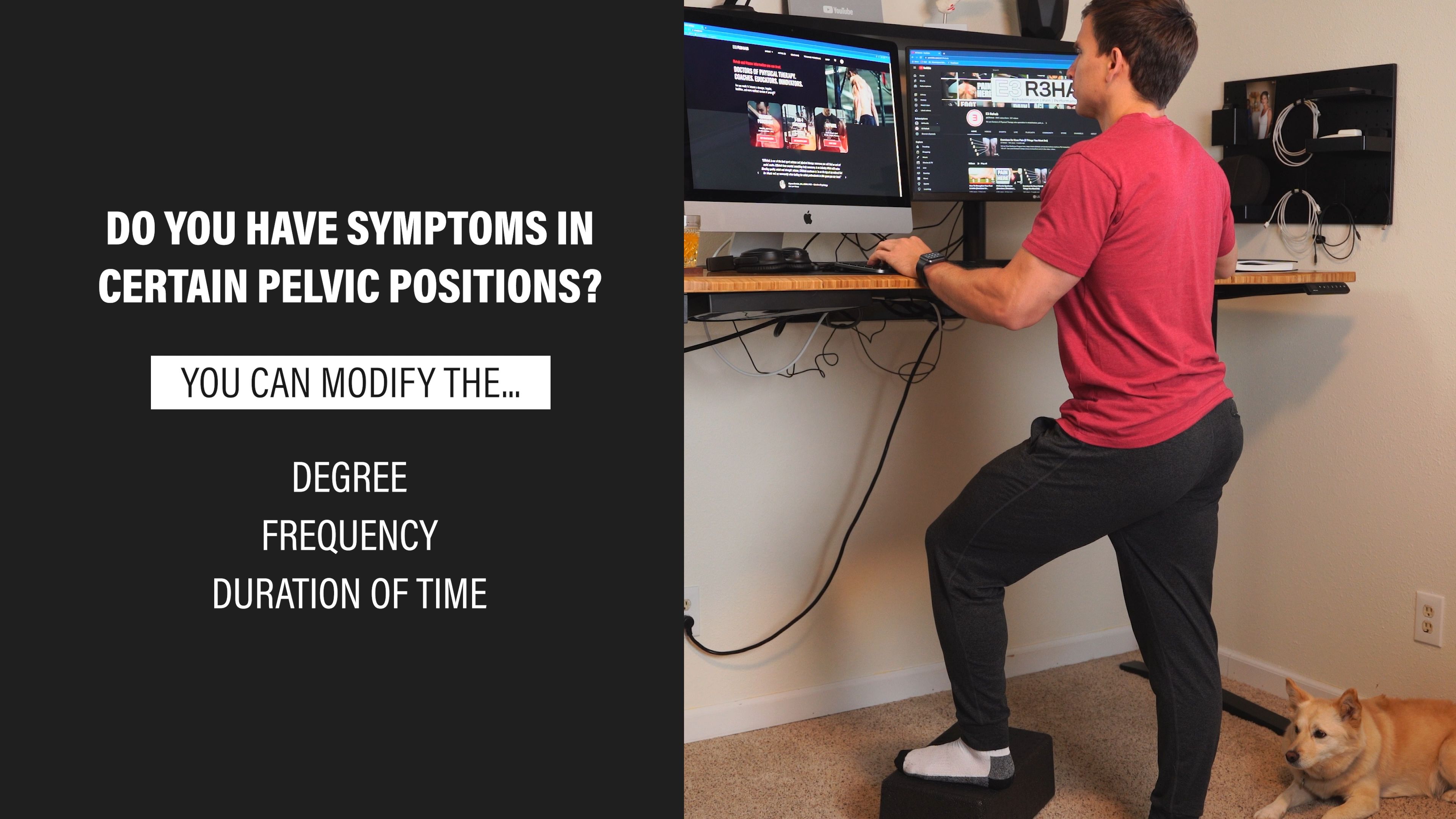
Does That Mean Anterior Pelvic Tilt Never Matters?
No, but we don’t need to vilify or demonize it because it’s no different than any other position or movement. If there are specific instances when modifying the degree, frequency, or duration of time spent in a certain pelvic position reduces your symptoms or helps you accomplish a task, I’m all for it.
But it is NOT a diagnosis. It’s normal.

And your static standing position is not reflective of the average position of your spine and pelvis throughout the day. For example, a study by Dreischarf et al in 2016 found that “Lumbar lordosis is not constant but rather is highly variable during the day, and on average, it is considerably smaller during the day than in standing position.”
What If You Want To Change For Aesthetic Reasons?
Meaning you don’t like the way it looks.
If you’re interested in changing your appearance, that’s completely up to you, but I think there’s 2 important things to consider:
- People create programs and videos to fix anterior pelvic tilt because they sell. If you look at popular rehab and fitness channels, their top viewed videos are related to fixing anterior pelvic tilt. Feeding into your insecurities and preying on those insecurities drive clicks and sales.
- Before and after pictures are deceitful. If you work with me and I tell you that you have anterior pelvic tilt, show you exercises to fix your anterior pelvic tilt, and then we reassess your standing posture, you’ll likely consciously or subconsciously make changes to meet my expectations of “good posture.” Also, Schmidt et al in 2018 found that repeated standing postures are actually quite variable.
What If Exercises Helped You?
I think that’s amazing, but that doesn’t mean we can conclude it’s because of your anterior pelvic tilt or because they fixed your anterior pelvic tilt. The exercises could be adding variability to your daily routine, contributing to less sedentary behavior, meeting your expectations and beliefs, or there’s a variety of other possible reasons.
Whatever the reason, continue the exercises if they’re helping you. I just don’t want you to stress about something that’s normal.
Final Thoughts
I know that some individuals might argue that it’s excessive anterior pelvic tilt that matters, but there’s huge variability in the shape of people’s pelvises and the usual measurements or estimations are actually unreliable.
If you disagree with any aspects of the blog, feel free to share your thoughts.
My primary purpose is to make you feel more confident, and help you understand how resilient and adaptable you are.
Looking for rehab or performance programs? Check out our store here!
Want to learn more? Check out some of our other similar blogs:
Exercise & Rehab Myths, Disc Herniations, Hip Pain
Thanks for reading. Check out the video and please leave any questions or comments below.


