The purpose of this blog is to debunk the 3 most common myths about leg length discrepancy, a finding in which one leg is a different length than the other.
Looking for rehab or performance programs? Check out our store here!
Myth #1: A Leg Length Difference Is The Cause of Pain
Let’s say you are experiencing back pain, see a clinician, and they find that one leg is longer than the other. They conclude that a leg length discrepancy is why you have pain. Seems reasonable, right?
Unfortunately, it’s not that simple. Here are 3 things to consider.
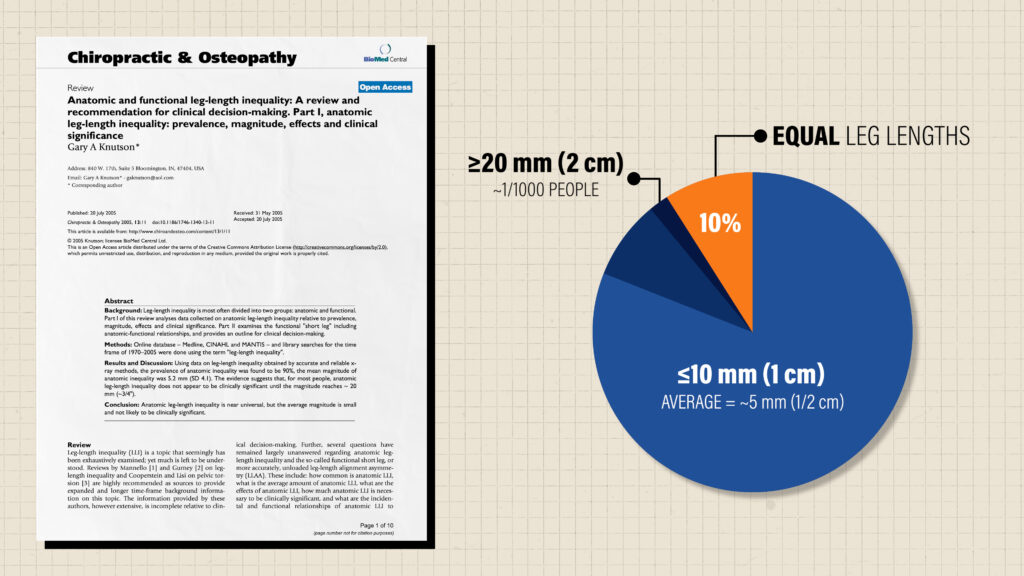
First, despite common beliefs, leg length discrepancies are actually very common.
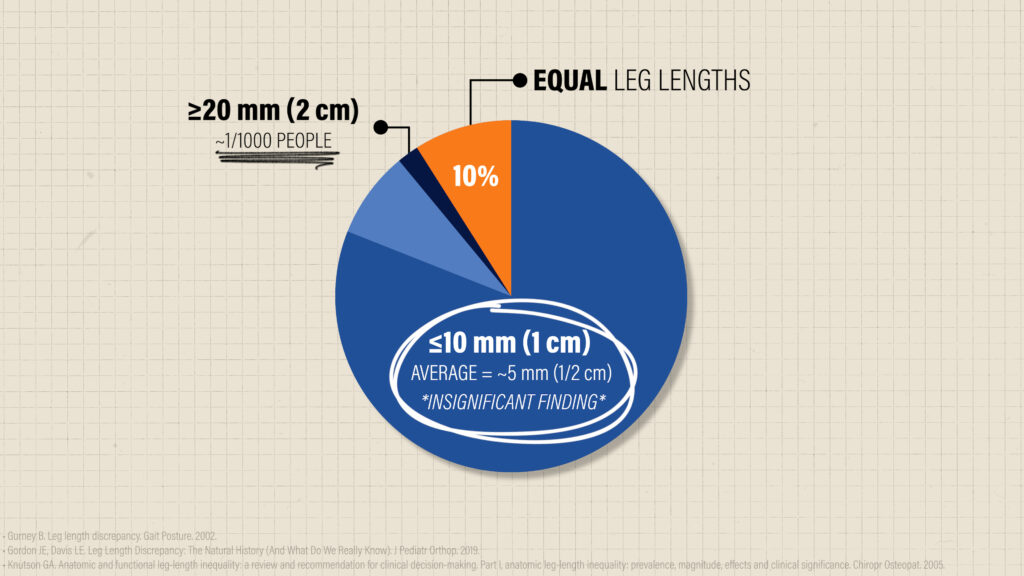
In a 2005 review, it was found that only around 10% of people have equal leg lengths. Of the remaining population, approximately 90% has a 10 mm, or 1 cm, discrepancy or less, with the average being roughly 5 mm, or ½ c. Larger differences are rare. For context, only about 1 in 1000 people reading this blog will have a difference over 20 mm, or 2 cm.
Second, leg length discrepancies have been shown to have a poor relationship with symptoms.
For example, Soukka et al. found that the “association between mild leg-length inequality and low back pain is questionable”, while other prospective studies found “no association”, or “no correlation”.
Gibson et al. in 1983 examined 15 patients at least a decade after acquiring a leg length difference (range 1.5-5.5 cm) as a result of a femoral fracture. The authors found that “no patients complained of low back pain nor had any had significant back pain during the previous 10 years.”
Lederman 2011 summarizes it best: “structural asymmetries are normal variations” that “cannot predict back pain and are unlikely to be its cause.”
Can a leg length difference lead to future pathology?
While some research might claim there is a connection between leg length discrepancies and other lower extremity pathologies, such as osteoarthritis, a 2002 review concluded that “any articles that find associations between LLD and pathological conditions must be interpreted with caution, as association does not prove a cause-effect relationship, and may just represent a coincident finding.”
As I will discuss in a bit, this doesn’t mean leg length differences are always irrelevant or your pain isn’t real. We just don’t have enough support to single out this finding as the sole reason for current or future symptoms.
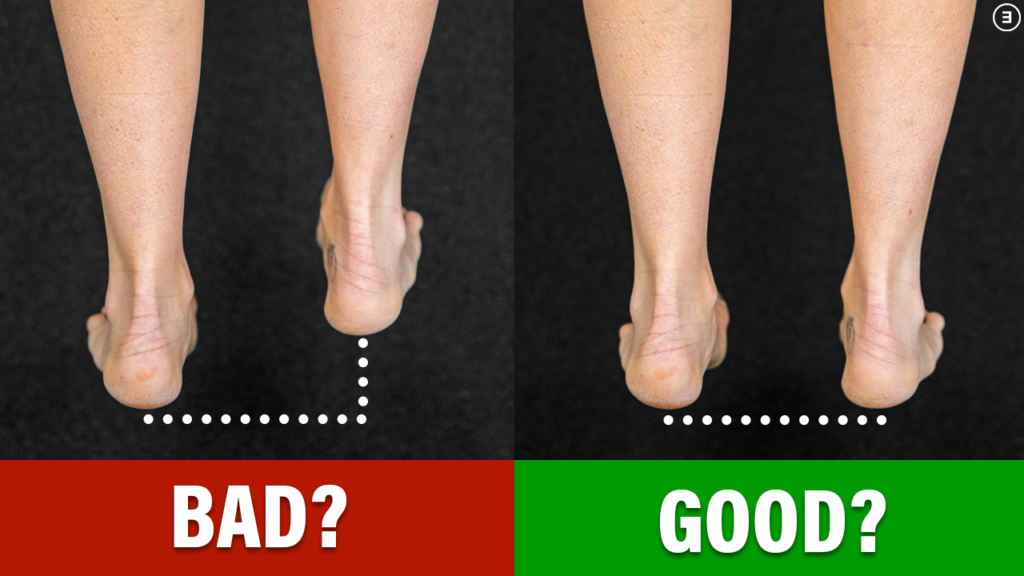
Third, measurement methods matter.
Did the clinician use a tape measure, blocks to attempt to “level” your pelvis, or just use their hands? Although common techniques, none of these have been proven to be effective. (Gibbons et al. 2002, Cooperstein et al. 2017, Sabharwal et al. 2008).
One study found that during a standing assessment, examiners were “unable to reliably detect leg length discrepancies of 1 cm or less.” This is significant because as I just mentioned, that makes up the majority of people with a leg length difference.
A 2008 review concluded that these options might be “useful screening tools, but they are not as accurate as imaging modalities,” such as an X-ray or CT scan.
But just because you can see or objectively measure leg length differences does not necessarily mean there is a problem to fix. This leads us to the next myth.
Myth #2: You Need To Fix A Leg Length Difference
Because leg length discrepancies are nearly universal and the average is only about 5 mm, this finding is considered insignificant for most people.
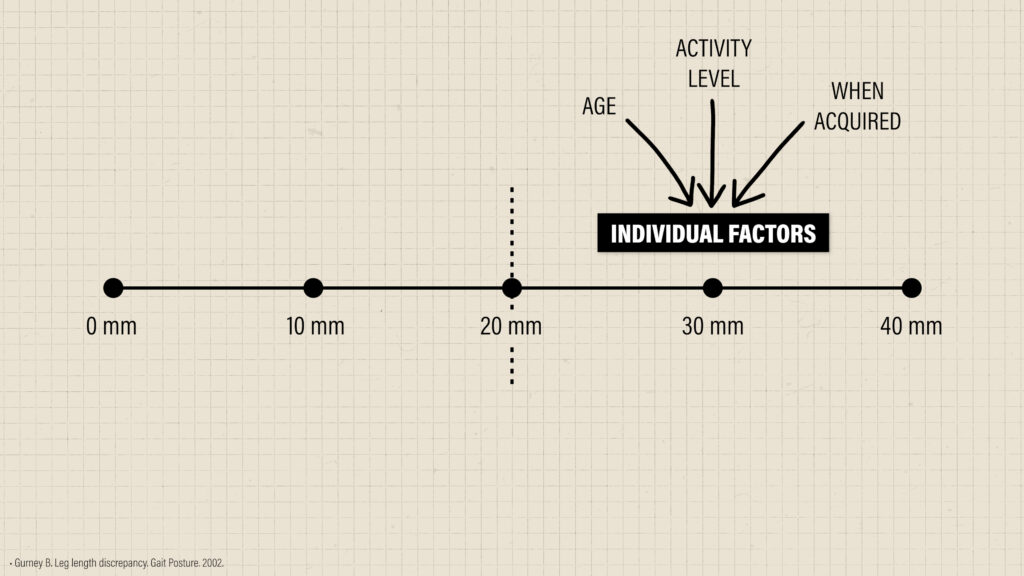
In some studies (Knuston 2005, Gordon 2019, Gurney 2002), it has been reported that roughly 20 mm is the threshold for when a discrepancy might become clinically meaningful. But as mentioned earlier, if you have a difference, odds are it will be less than 10 mm. A discrepancy above 20 mm is very rare.
Furthermore, the idea of a threshold should be interpreted with a grain of salt.
This doesn’t mean there is a hard cut-off that determines when a leg length discrepancy matters and doesn’t matter.
This information needs to be applied in the context of the individual, and factors such as age, activity level, and when the leg length was acquired are some considerations.
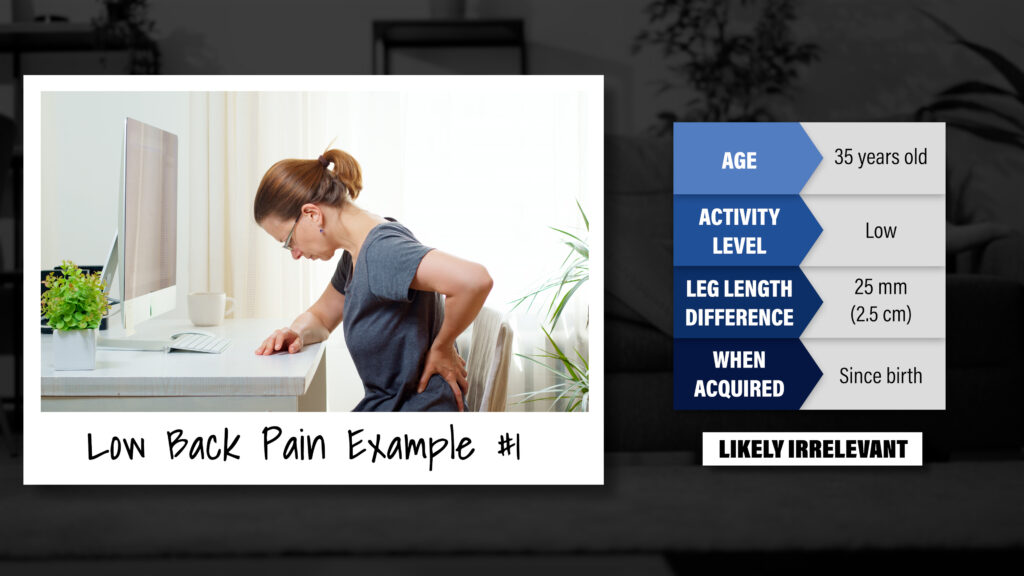
For example, if you’re a relatively inactive 35-year-old who has acute low back pain, a leg length discrepancy of 25 mm which you’ve had since birth is likely irrelevant since you would have adapted to this difference over your lifetime.
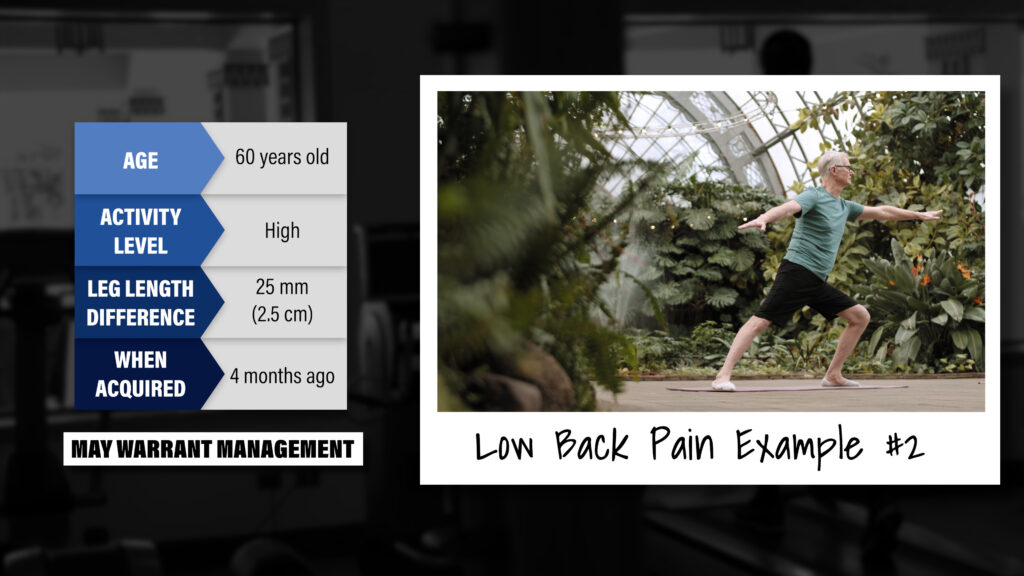
On the other hand, if you are an active 60-year-old who recently had a hip replacement that resulted in a 25 mm leg length difference, and are now experiencing new episodes of back pain, this large and sudden discrepancy may warrant management.
A common treatment option in this scenario might be using a shoe or heel lift.

A 2019 randomized control trial found that over the course of 12 months, a heel lift, compared to a regular insole, was an effective option for reducing low back pain in workers with a standing job.
In contrast, a 2018 systematic review concluded that “there is low-quality evidence that shoe lifts reduce pain and improve function in those with a leg length discrepancy.”
The research on this topic is mixed, but since heel lifts are generally low-cost and low-risk, it can be an option worth trying, especially if you have recently acquired a larger leg length difference and you suspect this to be a contributing factor to your symptoms.

Other treatments you might hear about are manual therapy techniques, stretches, or other “corrective” exercises.
While these may make you feel better, if a clinician claims these “fix” your leg length by “correcting” muscle imbalances or “realigning” your pelvis or spine, you should be skeptical.
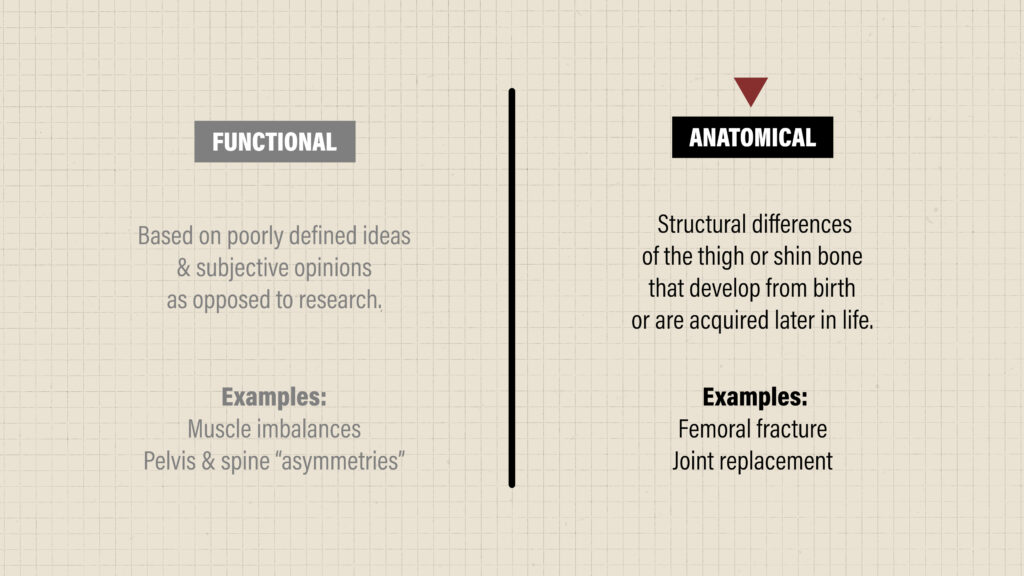
These are often claimed to treat a functional leg length difference which is based on poorly defined ideas and subjective opinion, as opposed to research. A true leg length discrepancy is most likely due to anatomical changes, which cannot be corrected by these treatments.
However, in most cases, you do not need to “ fix” a discrepancy. The human body is more than capable of tolerating such variations without a loss of function or developing future symptoms. As human beings, we are extremely resilient and adaptable.
Myth #3: Leg Length Differences Never Matter
Although rare, the populations of most interest are those who have acquired a large and sudden change in leg length difference, such as from a hip fracture or joint replacement, and are now experiencing a significant increase in pain and a decline in function.
In these cases, a heel lift can be a simple and inexpensive option for potentially reducing symptoms.
However, for a majority of people, leg length differences are not clinically significant, are not the cause of your pain, and do not require special treatment. They also should not stop you from doing what you want to do.
Do you want to lift weights? Play sports? Run?
In a 1983 paper, it was found that “discrepancies of 5 to 25 mm were not necessarily a functional detriment to marathon runners”.
It has also been reported that Usain Bolt has a 1.3 cm leg length difference. Video analysis showed that his right leg hit the ground with 13% more force and his left leg spent 14% more time on the ground. Clearly, his asymmetries did not impede his performance.
I have a leg length discrepancy in which my right leg is 15 mm, or 1.5 cm, longer than my left. I lift weights, run, play basketball, hike, and do a variety of other activities. It is not something that I let deter me from doing what I want to do.
It’s important to understand that a leg length discrepancy is a normal variation that has a poor relationship with pain, and is something that we can adapt to over time.
Summary
In summary, there are 3 common myths about leg length discrepancies:
Myth #1: A Leg Length Difference Is The Cause of Pain
- Fact #1 is that leg length discrepancies are very common and are shown to have a poor relationship with current and future symptoms. Any association with pain or other conditions should be interpreted with caution, as an association does not prove a cause-effect relationship and likely only represents a coincidental finding.
Myth #2: You Need To Fix A Leg Length Difference
- Fact #2 is that in most cases, leg length discrepancies are not a problem that needs to be “fixed” since human beings are adaptable and more than capable of tolerating such variations without experiencing a loss in function or symptoms.
Myth #3: Leg length Differences Never Matter
- Fact #3 is that although rare, a leg length difference can matter sometimes. However, for a majority of people, this is a normal variation that should not stop you from doing the activities you want to do.